Keenan Research Centre, St Michael's Hospital, Unity Health Toronto, 209 Victoria Street, Room 408, Toronto, ON, M5B 1T8, Canada.
Interdepartmental Division of Critical Care Medicine, University of Toronto, Toronto, Canada.
Intensive Care Med. 2022 Jul;48(7):888-898. doi: 10.1007/s00134-022-06724-y. Epub 2022 Jun 7.
In acute respiratory distress syndrome (ARDS), physiological parameters associated with outcome may help defining targets for mechanical ventilation. This study aimed to address whether transpulmonary pressures (P), including transpulmonary driving pressure (DP), elastance-derived plateau P, and directly-measured end-expiratory P, are better associated with 60-day outcome than airway driving pressure (DP). We also tested the combination of oxygenation and stretch index [PaO/(FiO*DP)].
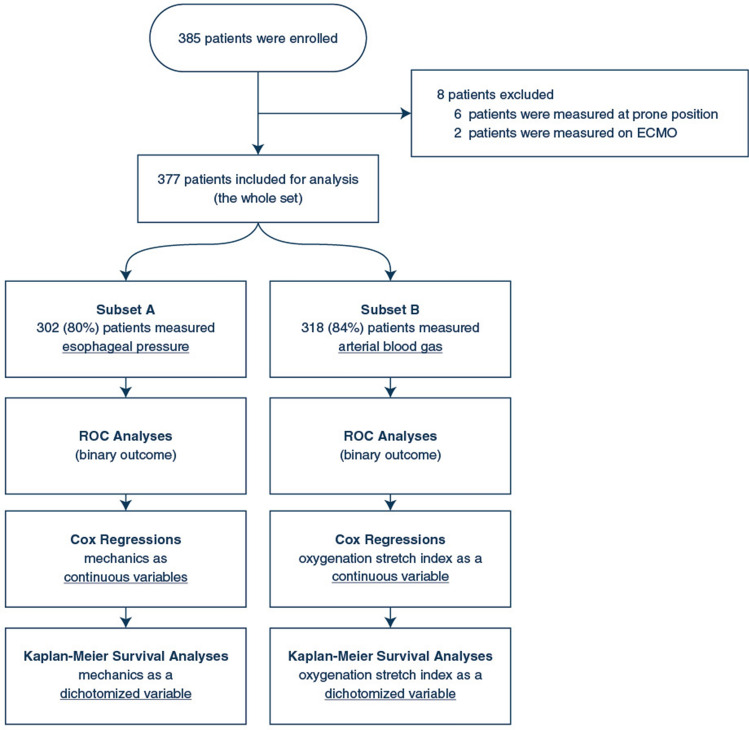
Prospective, observational, multicentre registry of ARDS patients. Respiratory mechanics were measured early after intubation at 6 kg/ml tidal volume. We compared the predictive power of the parameters for mortality at day-60 through receiver operating characteristic (ROC) and assessed their association with 60-day mortality through unadjusted and adjusted Cox regressions. Finally, each parameter was dichotomized, and Kaplan-Meier survival curves were compared.
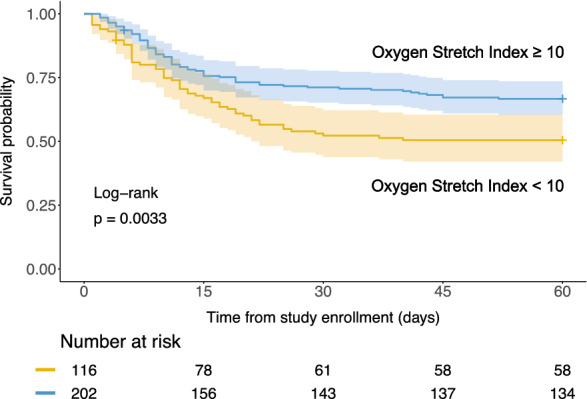
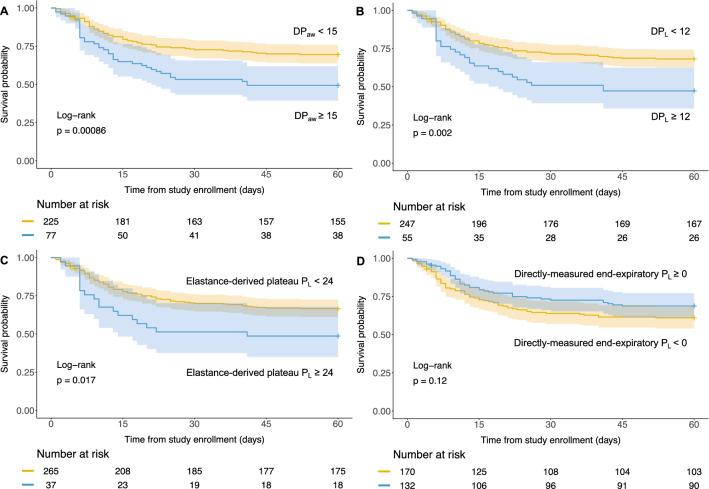
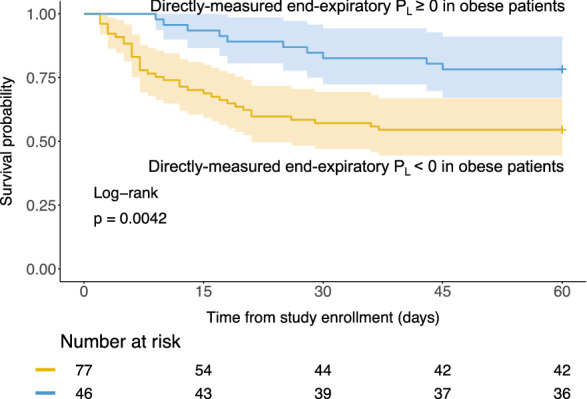
385 patients were enrolled 2 [1-4] days from intubation (esophageal pressure and arterial blood gases in 302 and 318 patients). As continuous variables, DP, DP, and oxygenation stretch index were associated with 60-day mortality after adjustment for age and Sequential Organ Failure Assessment, whereas elastance-derived plateau P was not. DP and DP performed equally in ROC analysis (P = 0.0835). DP had the best-fit Cox regression model. When dichotomizing the variables, DP ≥ 15, DP ≥ 12, plateau P ≥ 24, and oxygenation stretch index < 10 exhibited lower 60-day survival probability. Directly measured end-expiratory P ≥ 0 was associated with better outcome in obese patients.
DP was equivalent predictor of outcome than DP. Our study supports the soundness of limiting lung and airway driving pressure and maintaining positive end-expiratory P in obese patients.
在急性呼吸窘迫综合征(ARDS)中,与预后相关的生理参数可能有助于确定机械通气的目标。本研究旨在探讨跨肺压(P),包括跨肺驱动压(DP)、弹性衍生平台 P 和直接测量的呼气末 P,是否比气道驱动压(DP)更好地与 60 天预后相关。我们还测试了氧合和拉伸指数[PaO/(FiO*DP)]的组合。
前瞻性、观察性、ARDS 患者多中心登记研究。在 6ml/kg 潮气量插管后早期测量呼吸力学。我们通过接收者操作特征(ROC)比较参数对第 60 天死亡率的预测能力,并通过未调整和调整后的 Cox 回归评估它们与 60 天死亡率的关系。最后,将每个参数进行二分,并比较 Kaplan-Meier 生存曲线。
385 例患者在插管后 2[1-4]天入组(302 例和 318 例患者有食管压力和动脉血气)。作为连续变量,DP、DP 和氧合拉伸指数在调整年龄和序贯器官衰竭评估后与 60 天死亡率相关,而弹性衍生平台 P 则不相关。DP 和 DP 在 ROC 分析中表现相当(P=0.0835)。DP 具有最佳拟合 Cox 回归模型。当将变量二分时,DP≥15、DP≥12、平台 P≥24 和氧合拉伸指数<10 表现出较低的 60 天生存率。直接测量的呼气末 P≥0 与肥胖患者的更好结局相关。
DP 与 DP 一样是预后的预测因子。我们的研究支持限制肺和气道驱动压并维持肥胖患者呼气末正压的合理性。