Department of Pharmacology, Ribeirao Preto Medical School, University of São Paulo, Brazil; Clinical and Experimental Sciences, Faculty of Medicine, University of Southampton, UK.
Clinical and Experimental Sciences, Faculty of Medicine, University of Southampton, UK.
Redox Biol. 2022 Aug;54:102362. doi: 10.1016/j.redox.2022.102362. Epub 2022 Jun 9.
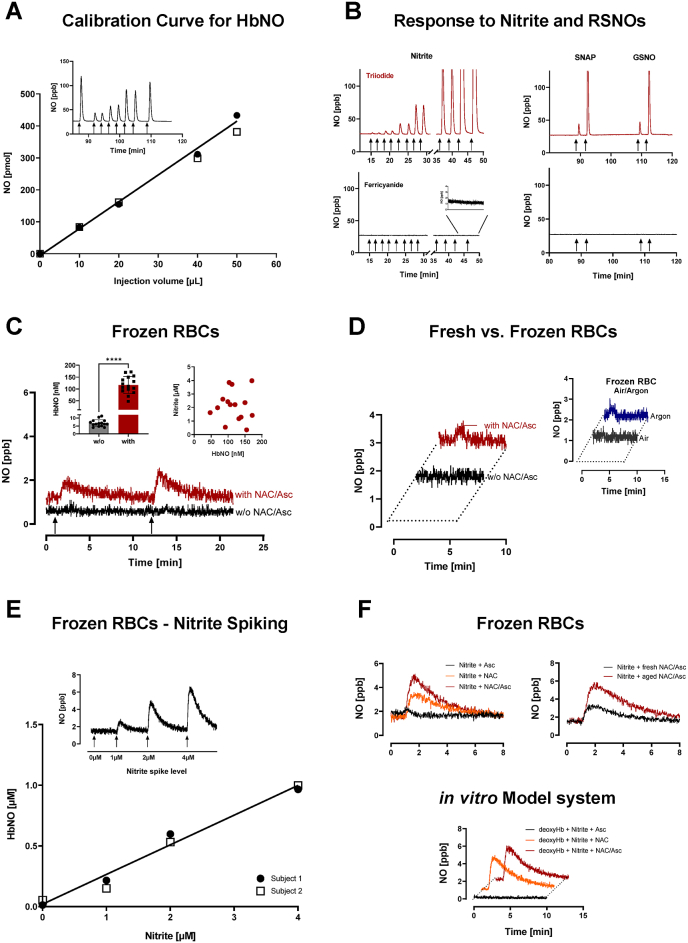
In blood, the majority of endothelial nitric oxide (NO) is scavenged by oxyhemoglobin, forming nitrate while a small part reacts with dissolved oxygen to nitrite; another fraction may bind to deoxyhemoglobin to generate nitrosylhemoglobin (HbNO) and/or react with a free cysteine to form a nitrosothiol. Circulating nitrite concentrations in healthy individuals are 200-700 nM, and can be even lower in patients with endothelial dysfunction. Those levels are similar to HbNO concentrations ([HbNO]) recently reported, whereby EPR-derived erythrocytic [HbNO] was lower in COVID-19 patients compared to uninfected subjects with similar cardiovascular risk load. We caution the values reported may not reflect true (patho)physiological concentrations but rather originate from complex chemical interactions of endogenous nitrite with hemoglobin and ascorbate/N-acetylcysteine. Using an orthogonal detection method, we find baseline [HbNO] to be in the single-digit nanomolar range; moreover, we find that these antioxidants, added to blood collection tubes to prevent degradation, artificially generate HbNO. Since circulating nitrite also varies with lifestyle, dietary habit and oral bacterial flora, [HbNO] may not reflect endothelial activity alone. Thus, its use as early marker of NO-dependent endothelial dysfunction to stratify COVID-19 patient risk may be premature. Moreover, oxidative stress not only impairs NO formation/bioavailability, but also shifts the chemical landscape into which NO is released, affecting its downstream metabolism. This compromises the endothelium's role as gatekeeper of tissue nutrient supply and modulator of blood cell function, challenging the body's ability to maintain redox balance. Further studies are warranted to clarify whether the nature of vascular dysfunction in COVID-19 is solely of endothelial nature or also includes altered erythrocyte function.
在血液中,大部分内皮一氧化氮(NO)被氧合血红蛋白清除,形成硝酸盐,而一小部分与溶解氧反应生成亚硝酸盐;另一部分可能与脱氧血红蛋白结合生成亚硝基血红蛋白(HbNO)和/或与游离半胱氨酸反应形成硫代亚硝基化合物。健康个体的循环亚硝酸盐浓度为 200-700 nM,内皮功能障碍患者的浓度甚至更低。这些水平与最近报道的 HbNO 浓度相似,其中 COVID-19 患者的 EPR 衍生红细胞 HbNO 浓度低于具有相似心血管风险负荷的未感染对照。我们提醒注意,报告的值可能无法反映真实的(病理)生理浓度,而可能源于内源性亚硝酸盐与血红蛋白和抗坏血酸/N-乙酰半胱氨酸的复杂化学相互作用。使用正交检测方法,我们发现基线 HbNO 处于个位数纳米摩尔范围;此外,我们发现这些抗氧化剂添加到血液采集管中以防止降解,会人为地产生 HbNO。由于循环亚硝酸盐也随生活方式、饮食习惯和口腔细菌菌群而变化,因此 HbNO 可能无法单独反映内皮活性。因此,将其用作分层 COVID-19 患者风险的 NO 依赖性内皮功能障碍的早期标志物可能还为时过早。此外,氧化应激不仅会损害 NO 的形成/生物利用度,还会改变 NO 释放的化学环境,影响其下游代谢。这会损害内皮作为组织营养供应的守门员和血细胞功能调节剂的作用,挑战身体维持氧化还原平衡的能力。需要进一步的研究来阐明 COVID-19 中血管功能障碍的性质是否仅为内皮性质,还是还包括改变的红细胞功能。