Esophagogastric Surgery Unit, Haut Lévêque Hospital, CHU Bordeaux, Bordeaux, France.
Thoracic Surgery Unit, Haut Lévêque Hospital, CHU Bordeaux, Bordeaux, France.
Surg Endosc. 2022 Oct;36(10):7266-7278. doi: 10.1007/s00464-022-09127-8. Epub 2022 Jun 22.
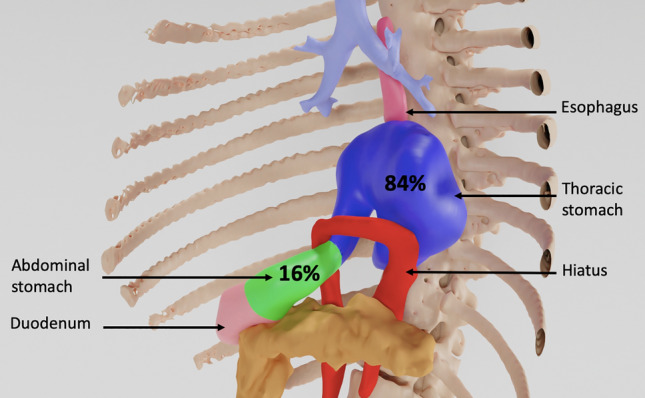
Dyspnoea in patients with a para-oesophageal hernia (PEH) occurs in 7% to 32% of cases and is very disabling, especially in elderly patients, and its origin is not well defined. The present study aims to assess the impact of PEH repair on dyspnoea and respiratory function.
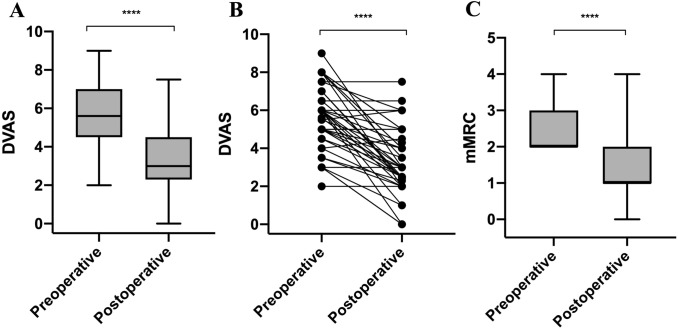
From January 2019 to May 2021, all consecutive patients scheduled for PEH repair presenting with a modified Medical Research Council (mMRC) score ≥ 2 for dyspnoea were included. Before and 2 months after surgery, dyspnoea was assessed by both the dyspnoea visual analogue scale (DVAS) and the mMRC scale, as well as pulmonary function tests (PFTs) by plethysmography.
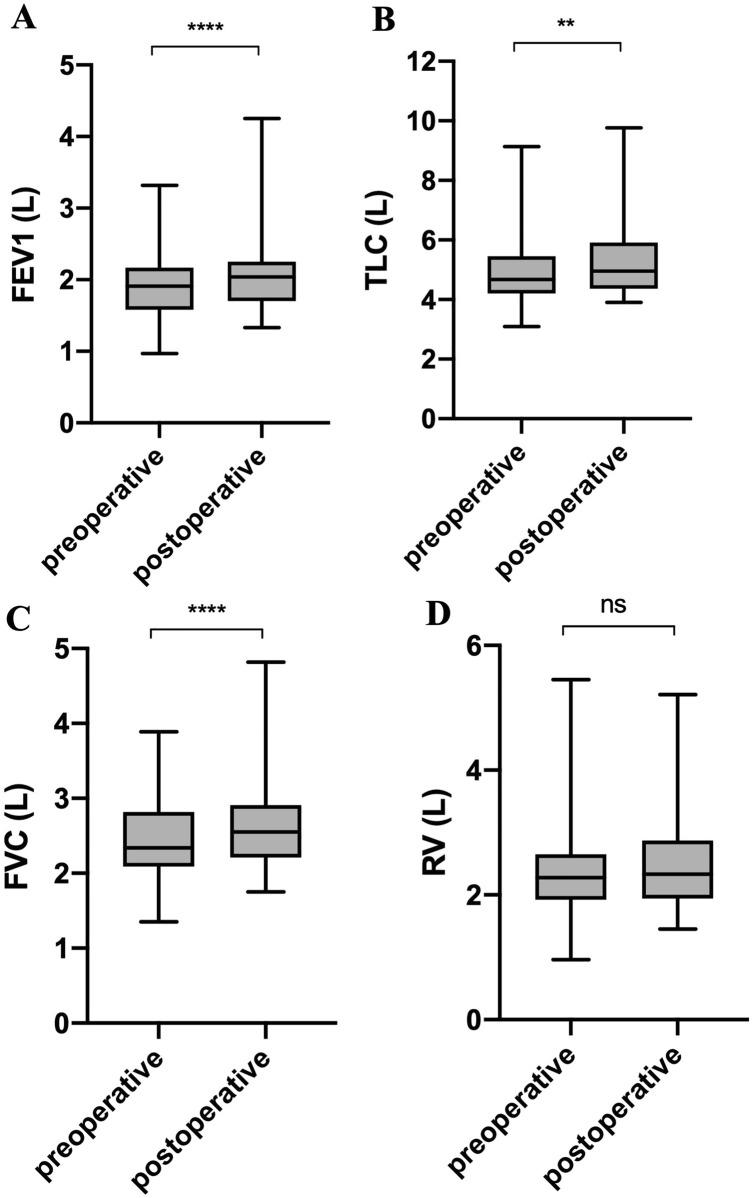
All 43 patients that were included had pre- and postoperative dyspnoea assessments and PFTs. Median age was 70 years (range 63-73.5 years), 37 (86%) participants were women, median percentage of the intrathoracic stomach was 59.9% (range 44.2-83.0%), and median length of hospital stay was 3 days (range 3-4 days). After surgery, the DVAS decreased statistically significant (5.6 [4.7-6.7] vs. 3.0 [2.3-4.4], p < 0.001), and 37 (86%) patients had a clinically significant decrease in mMRC score. Absolute forced expiratory volume in one second (FEV1), total lung capacity, and forced vital capacity also statistically significantly increased after surgery by an average of 11.2% (SD 17.9), 5.0% (SD 13.9), and 10.7% (SD 14.6), respectively. Furthermore, from the subgroup analysis, it was identified that patients with a lower preoperative FEV1 were more likely to have improvement in it after surgery. No correlation was found between improvement in dyspnoea and FEV1. There was no correlation between the percentage of intrathoracic stomach and dyspnoea or improvement in PFT parameters.
PEH repair improves dyspnoea and FEV1 in a statistically significant manner in a population of patients presenting with dyspnoea. Patients with a low preoperative FEV1 are more likely to have improvement in it after surgery.
食管旁疝(PEH)患者的呼吸困难发生率为 7%至 32%,且非常严重,尤其是在老年患者中,其发病机制尚不清楚。本研究旨在评估 PEH 修补术对呼吸困难和呼吸功能的影响。
2019 年 1 月至 2021 年 5 月,所有连续接受 PEH 修补术治疗且呼吸困难改良医学研究委员会(mMRC)评分≥2 分的患者均纳入本研究。术前和术后 2 个月,通过呼吸困难视觉模拟量表(DVAS)和 mMRC 量表以及体描法肺功能检查(PFT)评估呼吸困难。
43 例患者均完成术前和术后呼吸困难评估及 PFT 检查。患者中位年龄为 70 岁(范围 63-73.5 岁),37 例(86%)为女性,胸腔内胃的中位数百分比为 59.9%(范围 44.2-83.0%),中位住院时间为 3 天(范围 3-4 天)。术后,DVAS 显著下降(5.6[4.7-6.7] vs. 3.0[2.3-4.4],p<0.001),37 例(86%)患者 mMRC 评分显著降低。术后用力肺活量(FEV1)、肺总量和用力肺活量绝对值也分别平均增加了 11.2%(SD 17.9)、5.0%(SD 13.9)和 10.7%(SD 14.6)。此外,亚组分析发现,术前 FEV1 较低的患者术后 FEV1 改善的可能性更大。呼吸困难的改善与 FEV1 之间无相关性。胸腔内胃的百分比与呼吸困难或 PFT 参数的改善均无相关性。
PEH 修补术可显著改善呼吸困难患者的呼吸困难和 FEV1,术前 FEV1 较低的患者术后 FEV1 改善的可能性更大。