High-Dependency Unit, Department of Clinical and Experimental Medicine, Careggi University Hospital, Lg. Brambilla 3, 50134, Florence, Firenze, Italy.
Intern Emerg Med. 2022 Oct;17(7):2093-2101. doi: 10.1007/s11739-022-03016-7. Epub 2022 Jun 22.
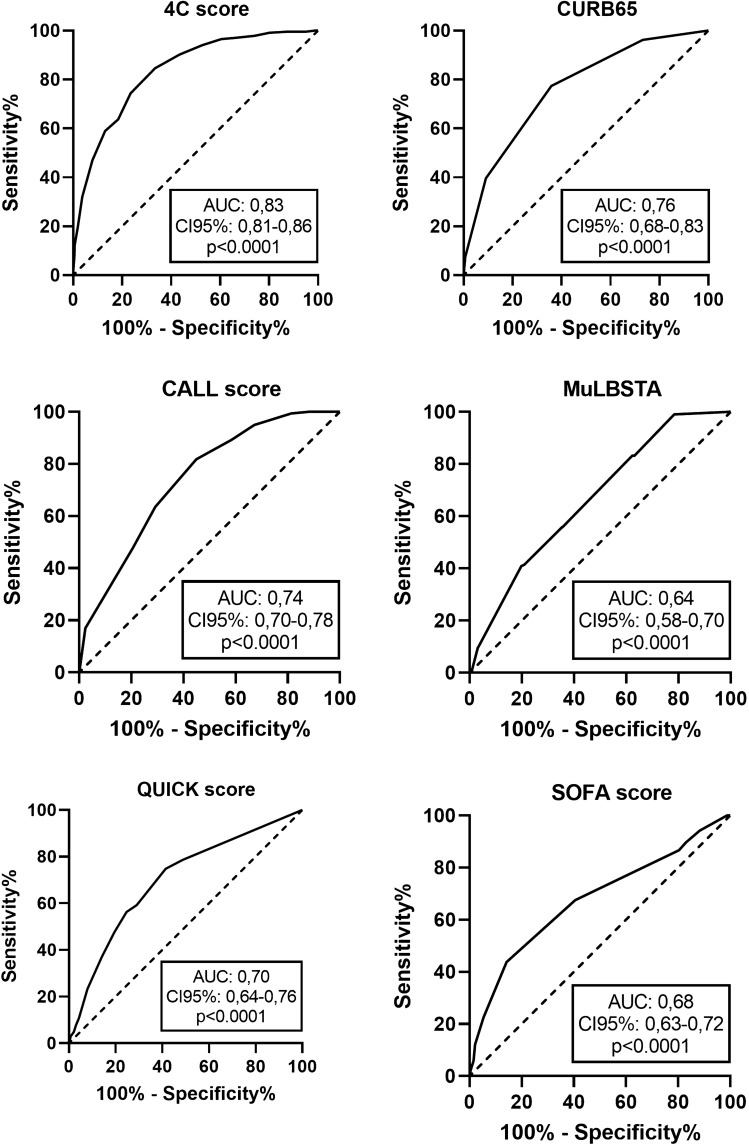
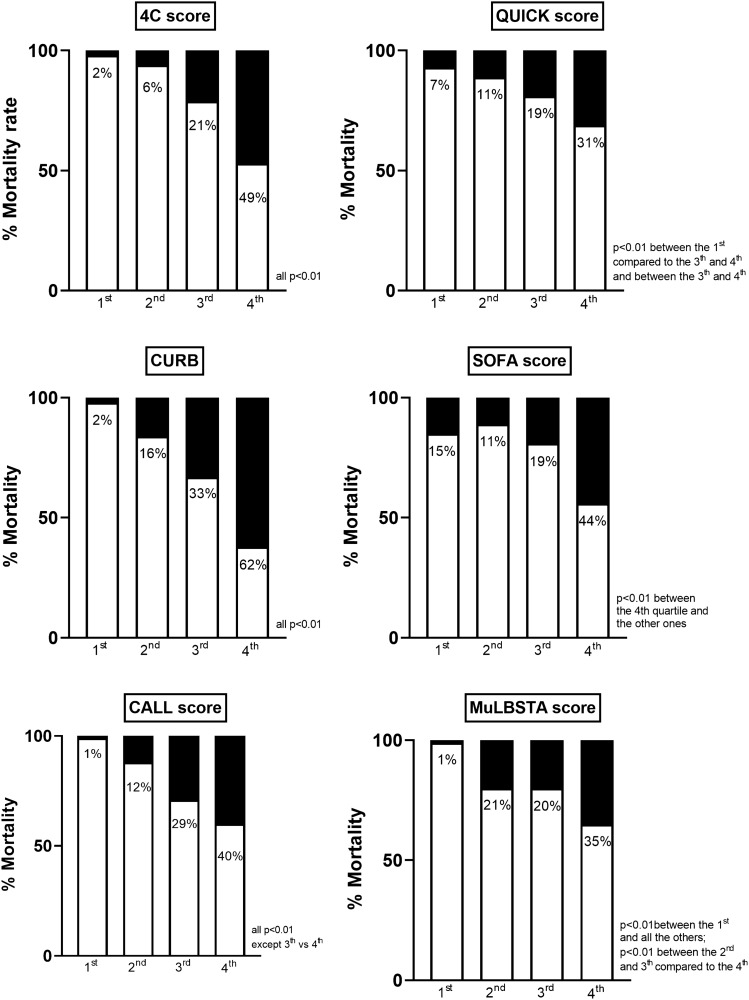
To test the prognostic performance of different scores, both specifically designed for patients with COVID-19 and generic, in predicting in-hospital mortality and the need for mechanical ventilation (MV). We retrospectively collected clinical data of patients admitted to the Emergency Department of the University Hospital AOU Careggi, Florence, Italy, between February 2020 and January 2021, with a confirmed infection by SARS-CoV2. We calculated the following scores: Sequential Organ Failure Assessment (SOFA) score, CALL score, 4C Mortality score, QUICK score, CURB-65 and MuLBSTA score. The end-points were in-hospital mortality and the need for MV. We included 1208 patients, mean age 60 ± 17 years, 57% male sex. Compared to survivors, non-survivors showed significantly higher values of all the prognostic scores (4C: 13 [10-15] vs 8 [4-10]; CALL: 11 [10-12] vs 9 [7-11]; QUICK: 4 [1-6] vs 0 [0-3]; SOFA: 5 [4-6] vs 4 [4-5]; CURB: 2 [1-3] vs 1 [0-1]; MuLBSTA: 11 [9-13] vs 9 [7-11], all p < 0.001). Discriminative ability evaluated by the Receiver Operating Curve analysis showed the following values of the Area under the Curve: 0.83 for 4C, 0.74 for CALL, 0.70 for QUICK, 0.68 for SOFA, 0.76 for CURB and 0.64 for MuLBSTA. The mortality rate significantly increased in increasing quartiles of 4C and CALL score (respectively, 2, 8, 24 and 54% for the 4C score and 1, 17, 33 and 68% for the CALL score, both p < 0.001). 4C and CALL score allowed an early and good prognostic stratification of patients admitted for pneumonia induced by SARS-CoV2.
为了测试专为 COVID-19 患者设计的和通用的不同评分系统在预测住院死亡率和机械通气(MV)需求方面的预后性能。我们回顾性地收集了 2020 年 2 月至 2021 年 1 月期间在意大利佛罗伦萨 AOU Careggi 大学医院急诊室收治的经 SARS-CoV2 感染确诊患者的临床数据。我们计算了以下评分:序贯器官衰竭评估(SOFA)评分、CALL 评分、4C 死亡率评分、QUICK 评分、CURB-65 评分和 MuLBSTA 评分。终点是住院死亡率和 MV 需求。我们纳入了 1208 名患者,平均年龄 60±17 岁,57%为男性。与幸存者相比,非幸存者的所有预后评分均显著更高(4C:13[10-15] 比 8[4-10];CALL:11[10-12] 比 9[7-11];QUICK:4[1-6] 比 0[0-3];SOFA:5[4-6] 比 4[4-5];CURB:2[1-3] 比 1[0-1];MuLBSTA:11[9-13] 比 9[7-11],均 P<0.001)。通过接受者操作特征曲线分析评估的区分能力显示了曲线下面积的以下值:4C 为 0.83,CALL 为 0.74,QUICK 为 0.70,SOFA 为 0.68,CURB 为 0.76,MuLBSTA 为 0.64。4C 和 CALL 评分的四分位值越高,死亡率显著增加(4C 评分分别为 2%、8%、24%和 54%,CALL 评分分别为 1%、17%、33%和 68%,均 P<0.001)。4C 和 CALL 评分能够对因 SARS-CoV2 引起的肺炎入院患者进行早期和良好的预后分层。