Yu Yingying, Wang Siyu, Su Nan, Pan Shida, Tu Bo, Zhao Jinfang, Shen Yingjuan, Qiu Qin, Liu Xiaomeng, Luan Junqing, Wang Fu-Sheng, Meng Fanping, Shi Ming
302 Clinical Medical School, Peking University, Beijing, China.
Senior Department of Infectious Diseases, The Fifth Medical Center of Chinese People's Liberation Army (PLA) General Hospital, Beijing, China.
Front Oncol. 2022 Jun 8;12:906824. doi: 10.3389/fonc.2022.906824. eCollection 2022.
Programmed cell death protein 1/programmed death-ligand 1 (PD-1/PD-L1) immune-related adverse events (irAEs) are inevitable in patients with liver cancer. Although the incidence of severe irAEs is low, but can result in fatal consequences. To date, only a few commonly used clinical biomarkers have been reported.
To assess commonly used clinical biomarkers associated with the occurrence of irAEs to enable better management of irAEs by clinicians.
We retrospectively reviewed patients with liver cancer treated with at least one cycle of PD-1 immune checkpoint inhibitors (ICIs) combined with tyrosine kinase inhibitors (TKIs). IrAEs were documented according to the common terminology criteria for adverse events version 5. Clinical and laboratory parameters were also evaluated.
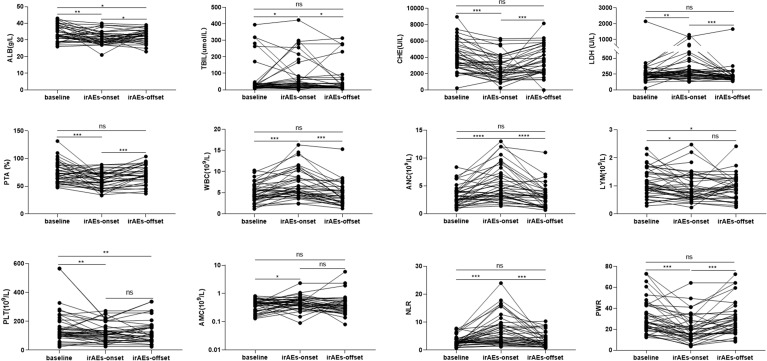
A total of 67 patients were included, 36 with irAEs and 31 without irAEs. A total of 104 adverse events occurred; 83 of these events were grade 1/2 (G1/G2), 21 were grade 3/4 (G3/G4), and one died of G4 hepatitis. Patients with irAEs had higher levels of C-reactive protein (CRP) and interleukin-6 (IL-6) and lower levels of lymphocyte subsets, except natural killer (NK) cell counts, than those without irAEs (0.05). Patients who experienced G3/G4 irAEs had higher levels of CRP and IL-6 and lower levels of CD4+ T lymphocytes and B lymphocytes than those who experienced G1/G2 irAEs (). Of note, impairments in liver function and routine blood tests were also observed . The results of univariate and multivariate analyses for any grade of irAEs revealed that the combination of sintilimab and lenvatinib ( 0.004, odds ratio [OR]: 7.414, 95% confidence interval [95% CI]: 1.925-28.560) and CRP ≥8.2 mg/L ( 0.024, OR: 3.727, CI: 1.185-11.726) were independent risk factors. Univariate and multivariate analyses of the risk factors of G3/G4 irAEs suggested that the combination of sintilimab and lenvatinib was a potential risk factor ( = 0.049, OR: 8.242, CI: 1.006-67.532).
Changes in patient CRP, IL-6, and lymphocyte subsets were associated with irAE onset and may act as potential biomarkers of irAEs. Impairments in liver function and routine blood tests owing to the occurrence of irAEs may become new concerns for clinicians.
程序性细胞死亡蛋白1/程序性死亡配体1(PD-1/PD-L1)免疫相关不良事件(irAEs)在肝癌患者中不可避免。虽然严重irAEs的发生率较低,但可导致致命后果。迄今为止,仅有少数常用的临床生物标志物被报道。
评估与irAEs发生相关的常用临床生物标志物,以便临床医生更好地管理irAEs。
我们回顾性分析了接受至少1个周期PD-1免疫检查点抑制剂(ICIs)联合酪氨酸激酶抑制剂(TKIs)治疗的肝癌患者。根据不良事件通用术语标准第5版记录irAEs。同时评估临床和实验室参数。
共纳入67例患者,36例发生irAEs,31例未发生irAEs。共发生104例不良事件;其中83例为1/2级(G1/G2),21例为3/4级(G3/G4),1例死于4级肝炎。与未发生irAEs的患者相比,发生irAEs的患者C反应蛋白(CRP)和白细胞介素-6(IL-6)水平较高,淋巴细胞亚群水平较低,但自然杀伤(NK)细胞计数除外(P<0.05)。发生G3/G4 irAEs的患者比发生G1/G2 irAEs的患者CRP和IL-6水平更高,CD4+T淋巴细胞和B淋巴细胞水平更低(P<0.05)。值得注意的是,还观察到肝功能和血常规检查出现异常。对任何级别的irAEs进行单因素和多因素分析的结果显示,信迪利单抗和仑伐替尼联合使用(P = 0.004,比值比[OR]:7.414,95%置信区间[95%CI]:1.925-28.560)以及CRP≥8.2 mg/L(P = 0.024,OR:3.727,CI:1.185-11.726)是独立危险因素。对G3/G4 irAEs的危险因素进行单因素和多因素分析表明,信迪利单抗和仑伐替尼联合使用是一个潜在危险因素(P = 0.049,OR:8.242,CI:1.006-67.532)。
患者CRP、IL-6和淋巴细胞亚群的变化与irAE的发生相关,可能作为irAEs的潜在生物标志物。由于irAEs的发生导致的肝功能和血常规检查异常可能成为临床医生新的关注点。