Diabetes Research Group, Cardiff University School of Medicine, Cardiff, UK.
All Wales Therapeutics and Toxicology Centre, The Routledge Academic Centre, University Hospital Llandough, Cardiff, UK.
Diabet Med. 2022 Sep;39(9):e14908. doi: 10.1111/dme.14908. Epub 2022 Jul 19.
There has been a dramatic increase in hypoglycaemic agent expenditure. We assessed the variability in prescribing costs at the practice level and the relationship between expenditure and the proportion of patients achieving target glycaemic control.
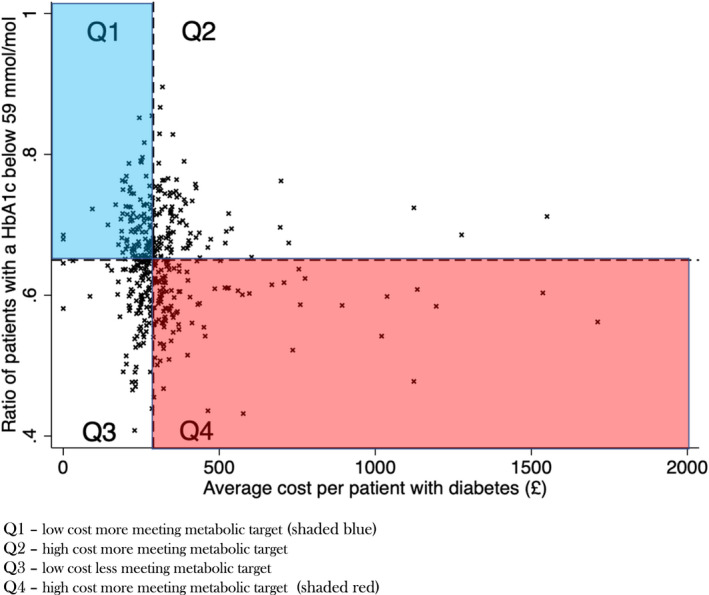
We utilized national prescribing data from 406 general practices in Wales. This was compared against glycaemic control (percentage of patients achieving a HbA1c level < 59 mmol/mol in the preceding 12 months). Analyses were adjusted for the number of patients with diabetes in each general practice and the Welsh Index of Multiple Deprivation.
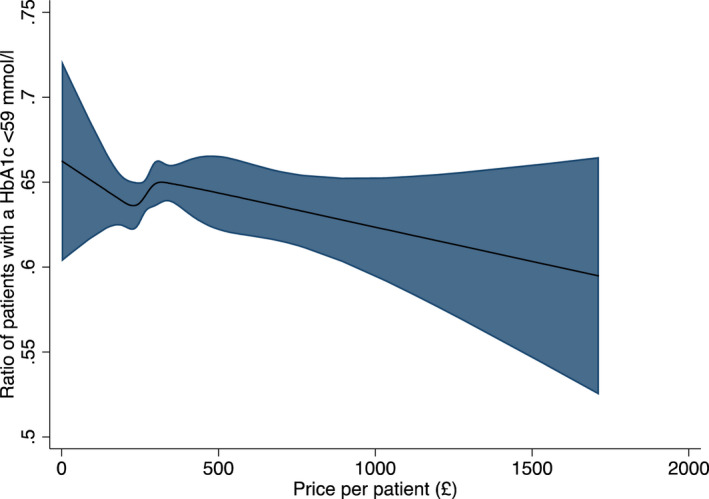
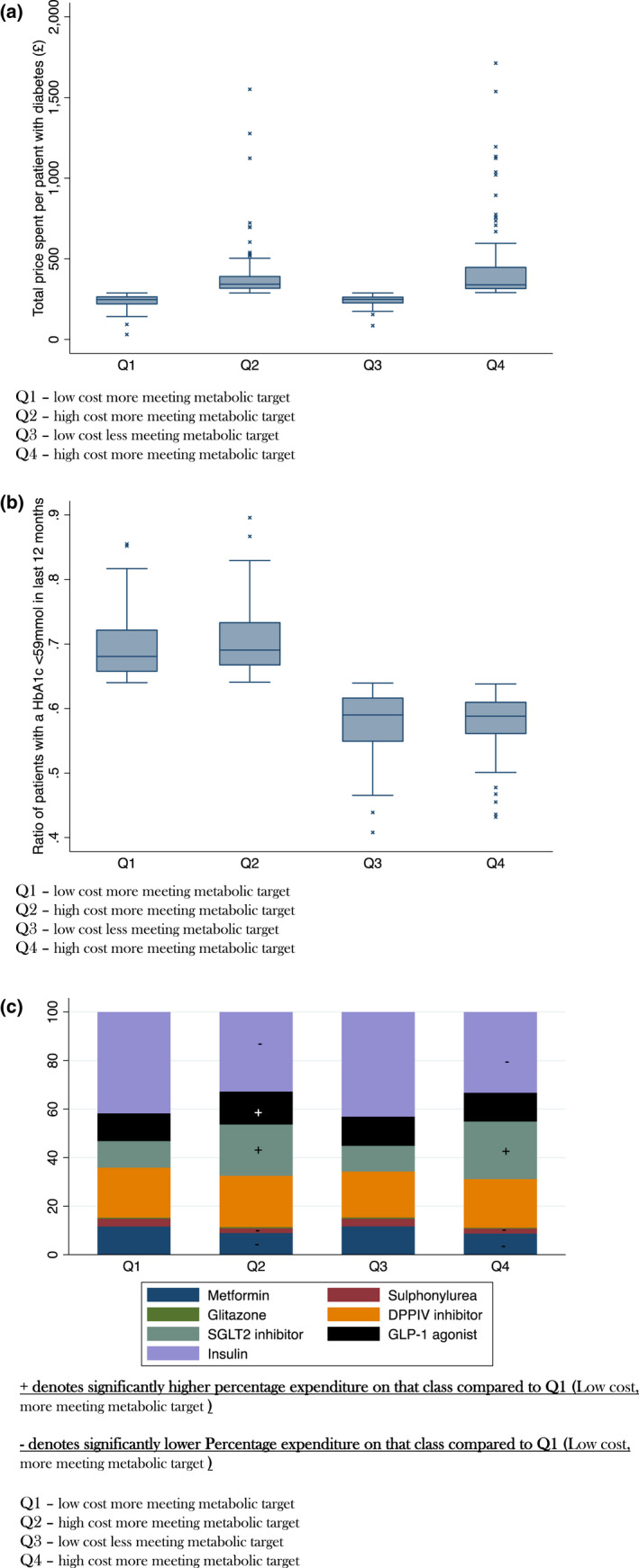
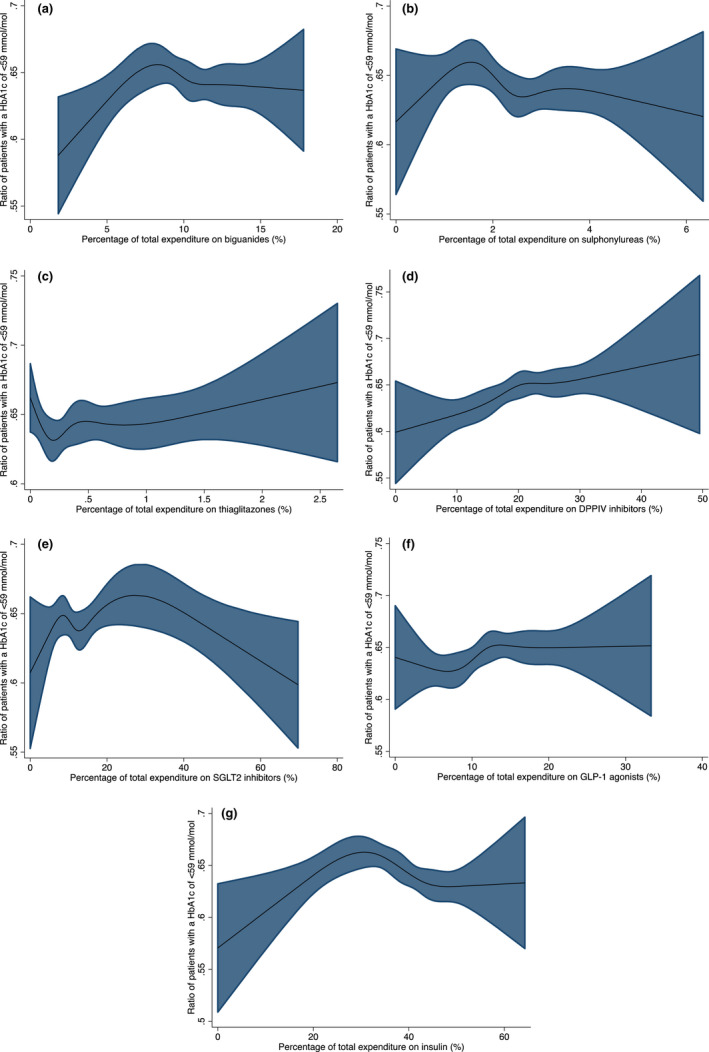
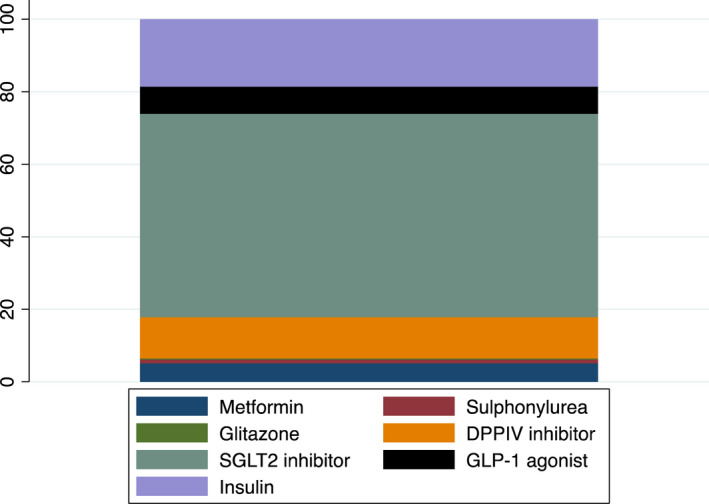
There was considerable heterogeneity in hypoglycaemic agent spend per patient with diabetes, Median = £289 (IQR 247-343) range £31.1-£1713. Higher total expenditure was not associated with improved glycaemic control B = -0.01 (95%CI -0.01, 0.002) p = 0.13. High-spend practices spent more on SGLT2 inhibitors (16 vs. 9% p < 0.001) and GLP-1 agonists (13 vs. 11% p < 0.001) and less on insulin (34 vs. 42% p < 0.001), biguanides (9 vs. 11% p = 0.001) and sulphonylureas (2 vs. 3% p < 0.001) than low spend practices. There were no differences in the pattern of drug prescribing between high spend practices with better glycaemic control (mean 68% of patients HbA1c <59 mmol/mol) and those with less good metabolic control (mean 58% of patients HbA1c <59 mmol/mol).
Spend on hypoglycaemic agents is highly variable between practices and increased expenditure per patient is not associated with better glycaemic control. Whilst newer, more expensive agents have additional benefits, in individuals where these advantages are more marginal widespread use of these agents has important cost implications.
降糖药物的支出大幅增加。我们评估了实践层面上的处方费用变化,并评估了支出与实现目标血糖控制的患者比例之间的关系。
我们利用威尔士 406 家普通诊所的全国处方数据。将这些数据与血糖控制(过去 12 个月内 HbA1c 水平<59mmol/mol 的患者比例)进行比较。分析调整了每个普通诊所的糖尿病患者人数和威尔士多重剥夺指数。
糖尿病患者的降糖药物人均支出存在很大差异,中位数为 289 英镑(IQR 247-343),范围为 31.1-1713 英镑。总支出较高与血糖控制的改善无关 B = -0.01(95%CI -0.01, 0.002)p = 0.13。高支出实践在 SGLT2 抑制剂(16%比 9%,p<0.001)和 GLP-1 激动剂(13%比 11%,p<0.001)上的花费更多,而在胰岛素(34%比 42%,p<0.001)、二甲双胍(9%比 11%,p=0.001)和磺脲类药物(2%比 3%,p<0.001)上的花费更少。在血糖控制较好(平均 68%的患者 HbA1c<59mmol/mol)和控制较差(平均 58%的患者 HbA1c<59mmol/mol)的高支出实践中,药物处方模式没有差异。
实践之间的降糖药物支出差异很大,每位患者的支出增加与血糖控制改善无关。虽然新型、更昂贵的药物有额外的好处,但在这些优势更为边缘的个体中,这些药物的广泛使用会带来重要的成本影响。