Department of Public Health, Policy and Systems, University of Liverpool, Liverpool, United Kingdom.
Medical University of Gdansk, Gdansk, Poland.
PLoS One. 2022 Jun 29;17(6):e0268766. doi: 10.1371/journal.pone.0268766. eCollection 2022.
There is uncertainty around the health impact and economic costs of the recent slowing of the historical decline in cardiovascular disease (CVD) incidence and the future impact on dementia and disability.
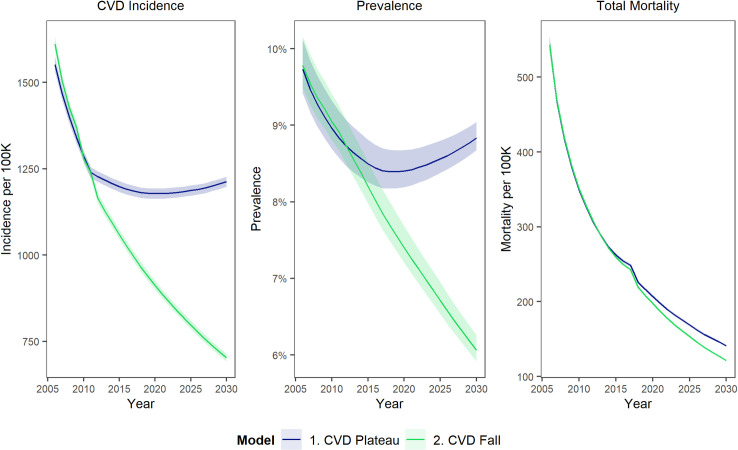
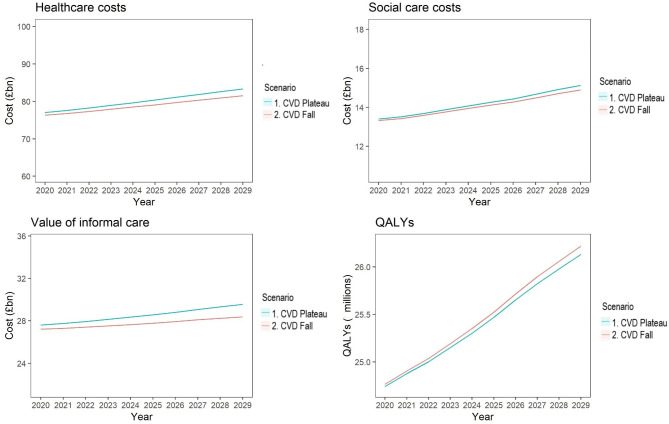
Previously validated IMPACT Better Ageing Markov model for England and Wales, integrating English Longitudinal Study of Ageing (ELSA) data for 17,906 ELSA participants followed from 1998 to 2012, linked to NHS Hospital Episode Statistics. Counterfactual design comparing two scenarios: Scenario 1. CVD Plateau-age-specific CVD incidence remains at 2011 levels, thus continuing recent trends. Scenario 2. CVD Fall-age-specific CVD incidence goes on declining, following longer-term trends. The main outcome measures were age-related healthcare costs, social care costs, opportunity costs of informal care, and quality adjusted life years (valued at £60,000 per QALY).
The total 10 year cumulative incremental net monetary cost associated with a persistent plateauing of CVD would be approximately £54 billion (95% uncertainty interval £14.3-£96.2 billion), made up of some £13 billion (£8.8-£16.7 billion) healthcare costs, £1.5 billion (-£0.9-£4.0 billion) social care costs, £8 billion (£3.4-£12.8 billion) informal care and £32 billion (£0.3-£67.6 billion) value of lost QALYs.
After previous, dramatic falls, CVD incidence has recently plateaued. That slowdown could substantially increase health and social care costs over the next ten years. Healthcare costs are likely to increase more than social care costs in absolute terms, but social care costs will increase more in relative terms. Given the links between COVID-19 and cardiovascular health, effective cardiovascular prevention policies need to be revitalised urgently.
心血管疾病(CVD)发病率近年来呈历史下降趋势,但近期出现放缓,这对痴呆症和残疾的未来影响存在不确定性,其健康影响和经济成本也不确定。
我们先前验证了用于英格兰和威尔士的 IMPACT Better Ageing 马尔可夫模型,该模型整合了 1998 年至 2012 年期间 17906 名参与英国老龄化纵向研究(ELSA)的参与者的 ELSA 数据,并与国民保健制度(NHS)医院发病统计数据相关联。该模型采用反事实设计,比较了两种情况:情况 1,CVD 稳定——特定年龄 CVD 发病率保持在 2011 年的水平,延续近期趋势;情况 2,CVD 下降——特定年龄 CVD 发病率继续下降,遵循长期趋势。主要结果测量指标是与年龄相关的医疗保健成本、社会护理成本、非正式护理的机会成本以及质量调整生命年(每 QALY 价值 60000 英镑)。
如果 CVD 持续稳定,在未来 10 年内,累计净货币成本约为 540 亿英镑(95%不确定性区间为 143 亿至 962 亿英镑),其中包括约 130 亿英镑(88 亿至 167 亿英镑)的医疗保健成本、15 亿英镑(-90 亿至 40 亿英镑)的社会护理成本、80 亿英镑(34 亿至 128 亿英镑)的非正式护理和 320 亿英镑(0.3 亿至 676 亿英镑)的 QALY 损失价值。
在之前大幅下降之后,CVD 发病率最近已趋于稳定。这种放缓可能会在未来十年内大幅增加医疗和社会护理成本。从绝对值来看,医疗保健成本的增长可能会超过社会护理成本,但从相对值来看,社会护理成本的增长幅度更大。鉴于 COVID-19 与心血管健康之间的联系,迫切需要重新激活有效的心血管预防政策。