Diaz Ashley A, Kubo Hana, Handa Nicole, Hanna Maria, Laronda Monica M
Stanley Manne Children's Research Institute, Ann & Robert H. Lurie Children's Hospital of Chicago, Chicago, IL, United States.
Feinberg School of Medicine, Northwestern University, Chicago, IL, United States.
Front Endocrinol (Lausanne). 2022 Jun 10;13:918899. doi: 10.3389/fendo.2022.918899. eCollection 2022.
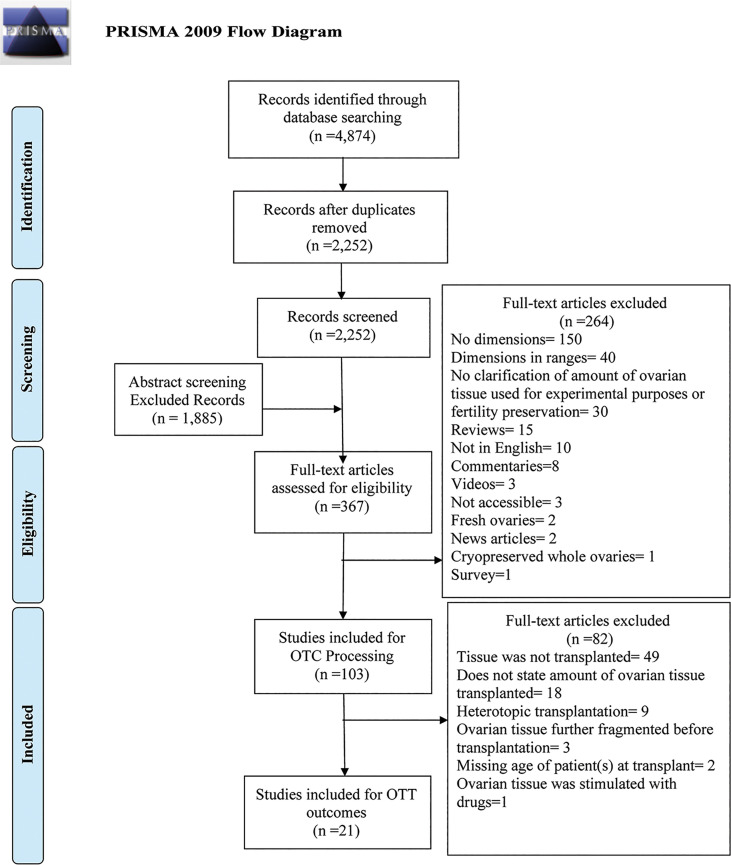
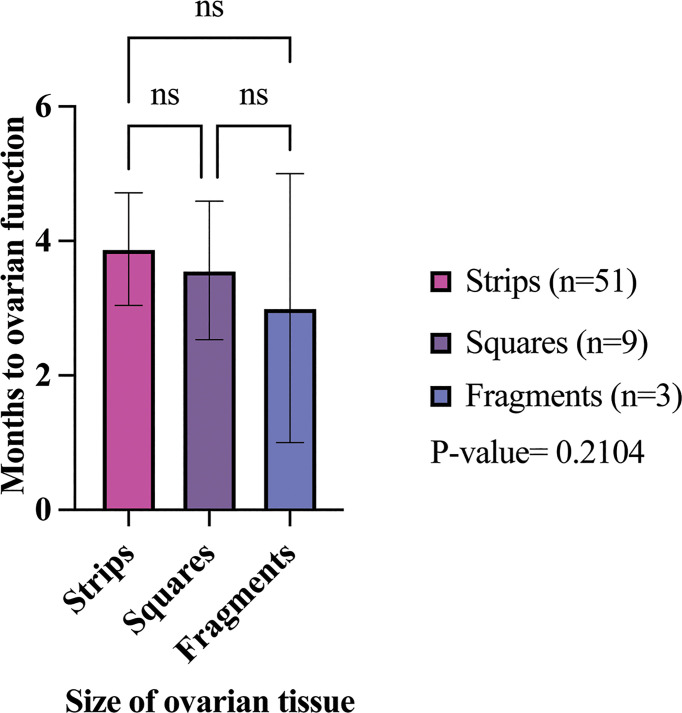
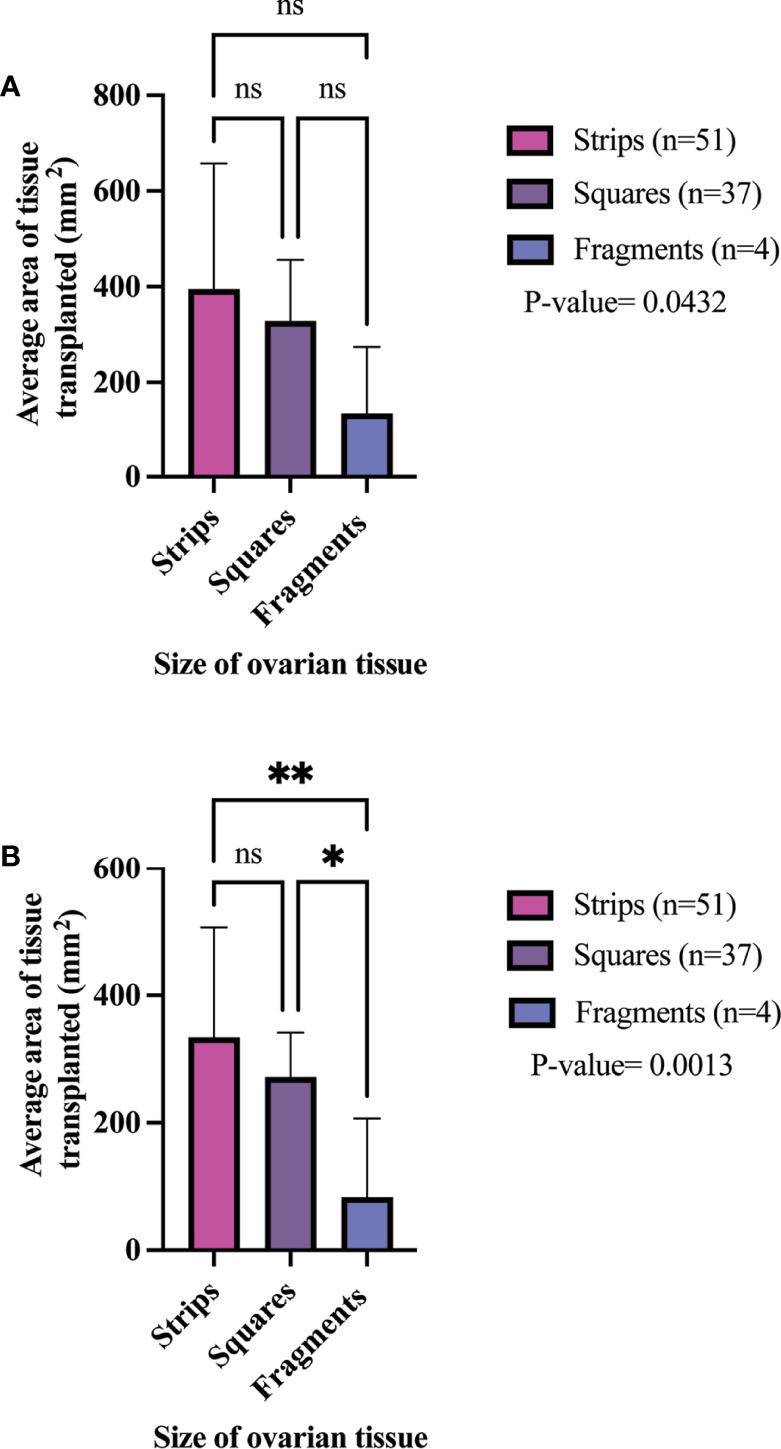
Ovarian tissue cryopreservation (OTC) is the only pre-treatment option currently available to preserve fertility for prepubescent girls and patients who cannot undergo ovarian stimulation. Currently, there is no standardized method of processing ovarian tissue for cryopreservation, despite evidence that fragmentation of ovaries may trigger primordial follicle activation. Because fragmentation may influence ovarian transplant function, the purpose of this systematic review was (1) to identify the processing sizes and dimensions of ovarian tissue within sites around the world, and (2) to examine the reported outcomes of ovarian tissue transplantation including, reported duration of hormone restoration, pregnancy, and live birth. A total of 2,252 abstracts were screened against the inclusion criteria. In this systematic review, 103 studies were included for analysis of tissue processing size and 21 studies were included for analysis of ovarian transplantation outcomes. Only studies where ovarian tissue was cryopreserved (via slow freezing or vitrification) and transplanted orthotopically were included in the review. The size of cryopreserved ovarian tissue was categorized based on dimensions into strips, squares, and fragments. Of the 103 studies, 58 fertility preservation sites were identified that processed ovarian tissue into strips (62%), squares (25.8%), or fragments (31%). Ovarian tissue transplantation was performed in 92 participants that had ovarian tissue cryopreserved into strips (n = 51), squares (n = 37), and fragments (n = 4). All participants had ovarian tissue cryopreserved by slow freezing. The pregnancy rate was 81.3%, 45.5%, 66.7% in the strips, squares, fragment groups, respectively. The live birth rate was 56.3%, 18.2%, 66.7% in the strips, squares, fragment groups, respectively. The mean time from ovarian tissue transplantation to ovarian hormone restoration was 3.88 months, 3.56 months, and 3 months in the strips, squares, and fragments groups, respectively. There was no significant difference between the time of ovarian function' restoration and the size of ovarian tissue. Transplantation of ovarian tissue, regardless of its processing dimensions, restores ovarian hormone activity in the participants that were reported in the literature. More detailed information about the tissue processing size and outcomes post-transplant are required to identify a preferred or more successful processing method.
[https://www.crd.york.ac.uk], identifier [CRD42020189120].
卵巢组织冷冻保存(OTC)是目前唯一可用于为青春期前女孩和无法进行卵巢刺激的患者保留生育能力的预处理方法。目前,尚无用于冷冻保存卵巢组织的标准化处理方法,尽管有证据表明卵巢破碎可能会触发原始卵泡激活。由于破碎可能会影响卵巢移植功能,本系统评价的目的是:(1)确定世界各地各机构卵巢组织的处理大小和尺寸;(2)研究卵巢组织移植报告的结果,包括报告的激素恢复持续时间、妊娠和活产情况。根据纳入标准共筛选了2252篇摘要。在本系统评价中,纳入103项研究分析组织处理大小,纳入21项研究分析卵巢移植结果。本评价仅纳入卵巢组织经冷冻保存(通过慢速冷冻或玻璃化)并原位移植的研究。将冷冻保存的卵巢组织大小按尺寸分为条带、方块和碎片。在103项研究中,确定了58个生育力保存机构,这些机构将卵巢组织处理成条带(62%)、方块(25.8%)或碎片(31%)。92名参与者接受了卵巢组织移植,其卵巢组织被冷冻保存成条带(n = 51)、方块(n = 37)和碎片(n = 4)。所有参与者的卵巢组织均通过慢速冷冻保存。条带组、方块组、碎片组的妊娠率分别为81.3%、45.5%、66.7%。条带组、方块组、碎片组的活产率分别为56.3%、18.2%、66.7%。从卵巢组织移植到卵巢激素恢复的平均时间,条带组为3.88个月,方块组为3.56个月,碎片组为3个月。卵巢功能恢复时间与卵巢组织大小之间无显著差异。文献报道中,无论卵巢组织的处理尺寸如何,其移植均可恢复参与者的卵巢激素活性。需要更多关于组织处理大小和移植后结果的详细信息,以确定更优或更成功的处理方法。