Vitti Emilia, Kim Ganghyun, Stockbridge Melissa D, Hillis Argye E, Faria Andreia V
Department of Neurology, School of Medicine, Johns Hopkins University, Baltimore, MD, United States.
Department of Neuroscience, Johns Hopkins University, Baltimore, MD, United States.
Front Neurol. 2022 Jun 14;13:912782. doi: 10.3389/fneur.2022.912782. eCollection 2022.
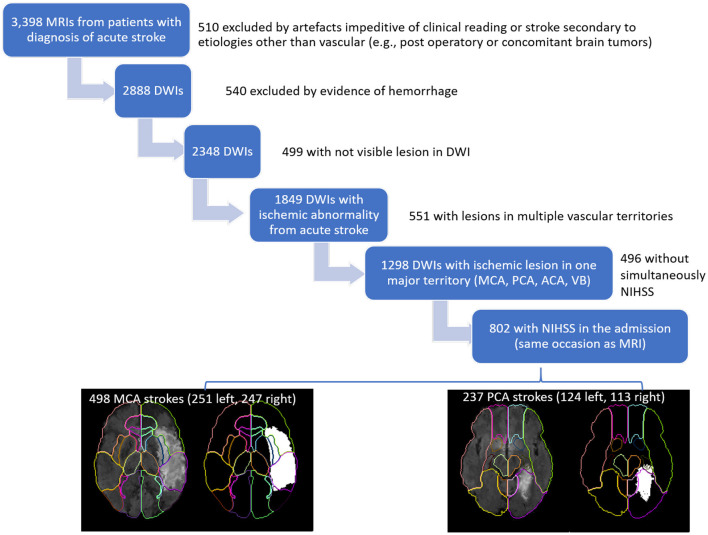
NIHSS score is higher for left vs. right hemisphere strokes of equal volumes. However, differences in each vascular territory have not been evaluated yet. We hypothesized that left vs. right differences are driven by the middle cerebral artery (MCA) territory, and there is no difference between hemispheres for other vascular territories. This study is based on data from 802 patients with evidence of acute ischemic stroke in one major arterial territory (MCA, = 437; PCA, = 209; ACA, = 21; vertebrobasilar, = 46). We examined differences in patients with left or right strokes regarding to lesion volume, NIHSS, and other covariates (age, sex, race). We used linear models to test the effects of these covariates on NIHSS. We looked at the whole sample as well as in the sample stratified by NIHSS (≤5 or >5) and by lesion location (MCA or PCA). Patients with left MCA strokes had significantly higher NIHSS than those with right strokes. Only patients with MCA strokes showed NIHSS score affected by the hemisphere when controlling for stroke volume and patient's age. This difference was driven by the more severe strokes (NIHSS>5). It is important to consider this systematic bias in the NIHSS when using the score for inclusion criteria for treatment or trials. Patients with right MCA stroke may be under-treated and left with disabling deficits that are not captured by the NIHSS.
在梗死体积相同的情况下,左半球卒中的美国国立卫生研究院卒中量表(NIHSS)评分高于右半球卒中。然而,尚未评估每个血管区域的差异。我们推测,左右半球之间的差异是由大脑中动脉(MCA)区域驱动的,而其他血管区域的半球之间没有差异。本研究基于802例在一个主要动脉区域(MCA,n = 437;PCA,n = 209;ACA,n = 21;椎基底动脉,n = 46)有急性缺血性卒中证据的患者的数据。我们检查了左、右半球卒中患者在梗死体积、NIHSS评分和其他协变量(年龄、性别、种族)方面的差异。我们使用线性模型来测试这些协变量对NIHSS评分的影响。我们观察了整个样本以及按NIHSS评分(≤5或>5)和梗死部位(MCA或PCA)分层的样本。左MCA卒中患者的NIHSS评分显著高于右MCA卒中患者。在控制梗死体积和患者年龄时,只有MCA卒中患者的NIHSS评分受半球影响。这种差异是由更严重的卒中(NIHSS>5)驱动的。在将NIHSS评分用作治疗或试验的纳入标准时,考虑这种系统偏差很重要。右MCA卒中患者可能未得到充分治疗,从而遗留NIHSS评分未能反映出的致残性缺陷。