Sorbonne Université, INSERM, Institut Pierre Louis d'Epidémiologie et de Santé Publique, Paris, France.
INSERM, Institut Pierre Louis d'Epidémiologie et de Santé Publique, AP-HP, Hôpital Pitié Salpêtrière, Département de Santé Publique, Centre de Pharmacoépidémiologie (Cephepi), Sorbonne Université, Paris, France.
J Eur Acad Dermatol Venereol. 2022 Nov;36(11):2101-2112. doi: 10.1111/jdv.18409. Epub 2022 Jul 22.
Biologics are the cornerstone of treatment of patients with moderate-to-severe plaque psoriasis and switches between biologics are frequently needed to maintain clinical improvement over time.
The main purpose of this study was to describe precisely switches between biologics and how their pattern changed over time with the recent availability of new biologic agents.
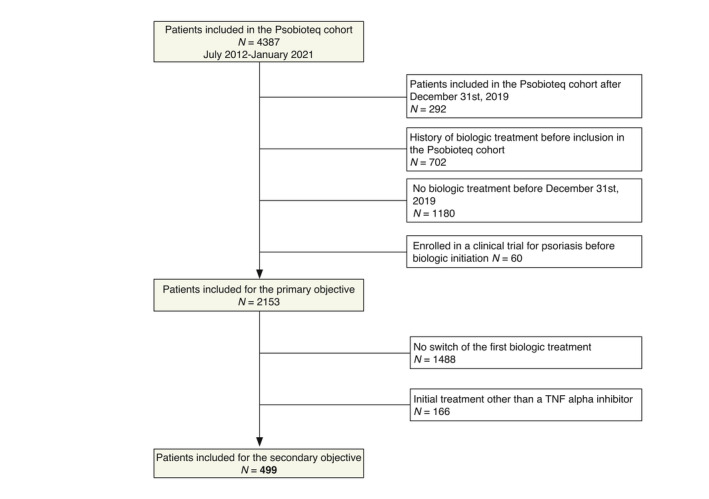
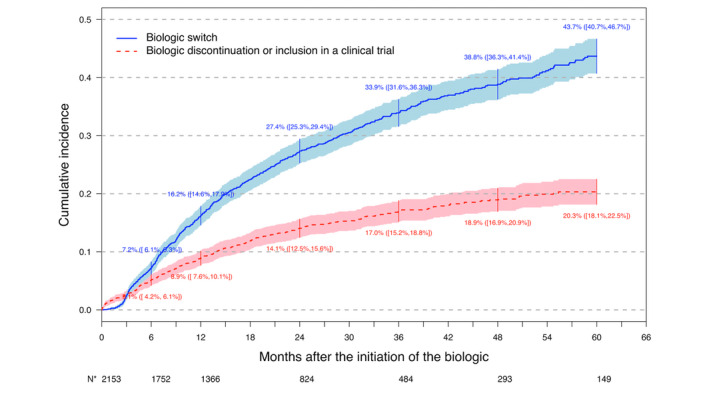
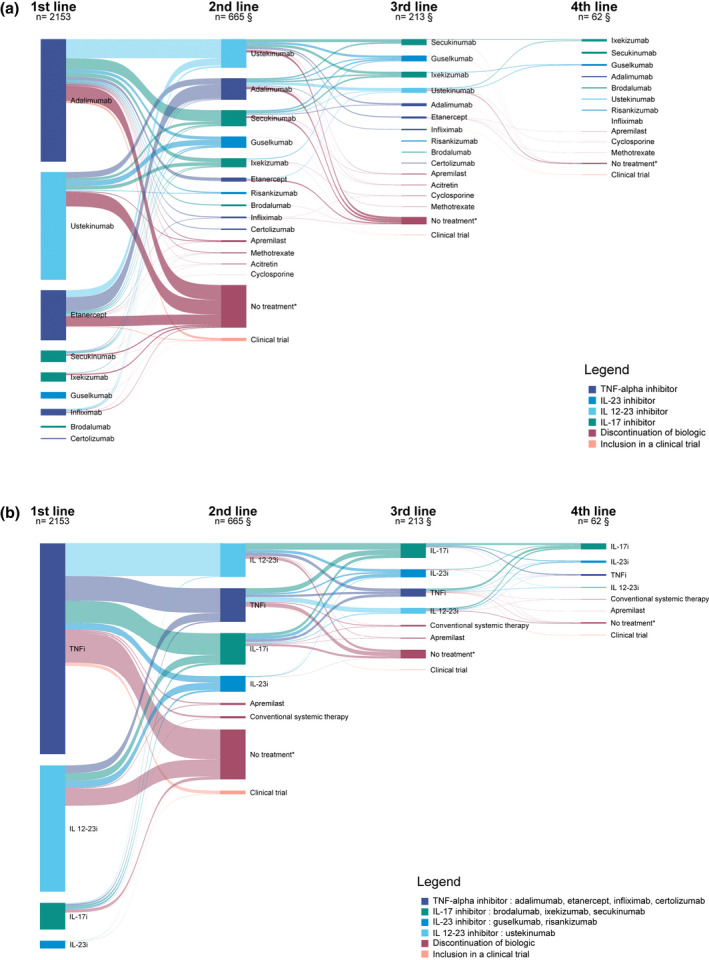
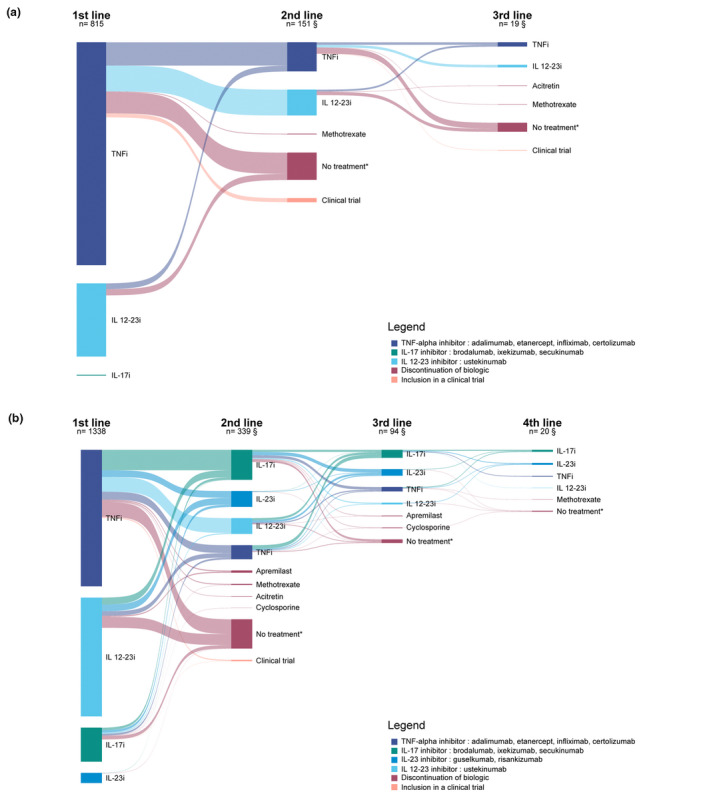
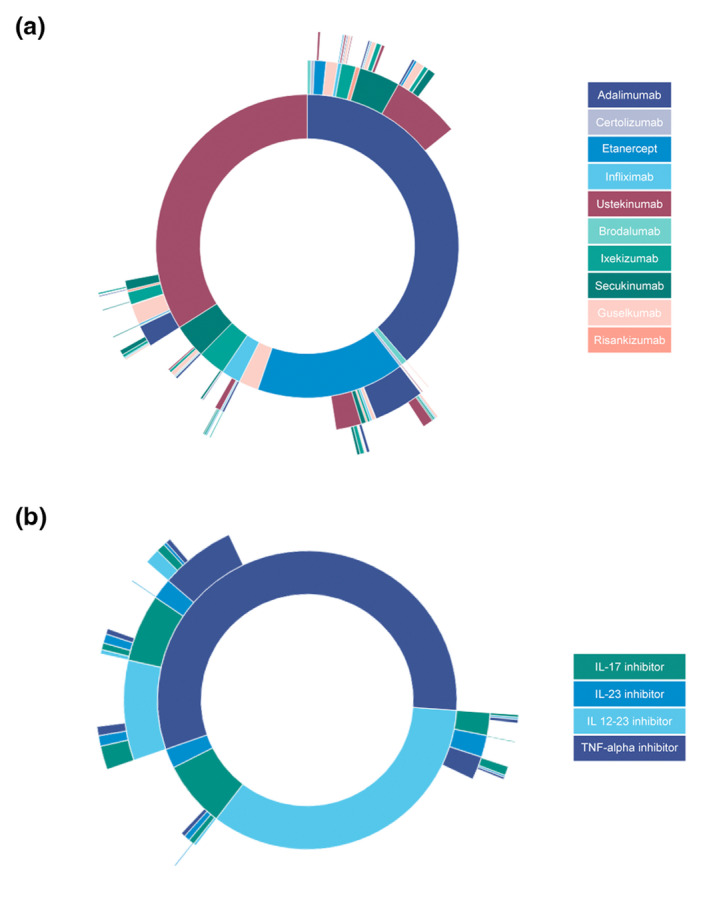
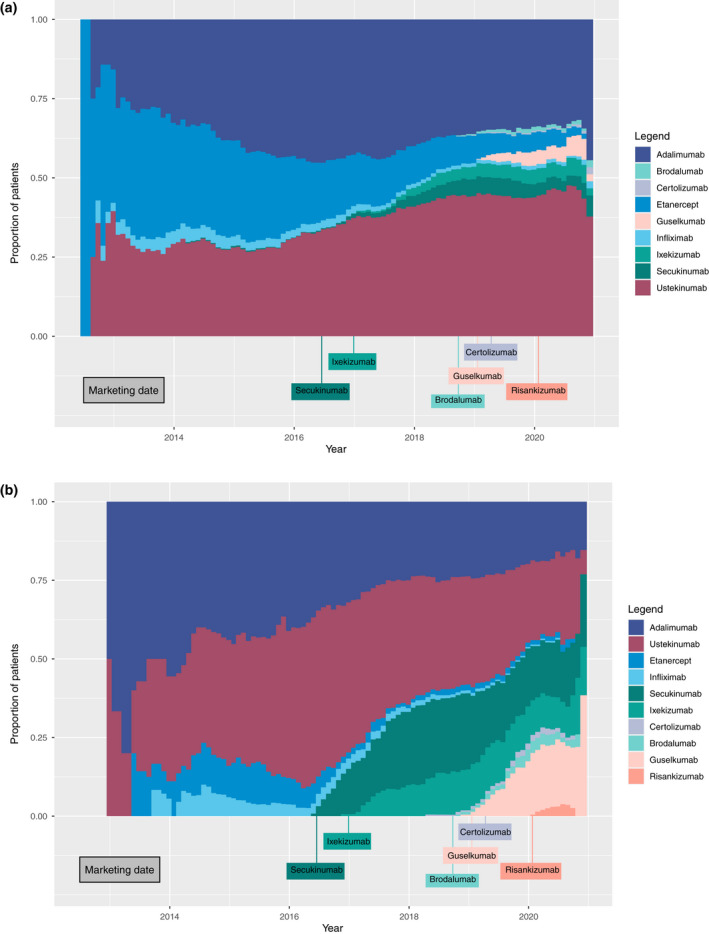
We included patients receiving a first biologic agent in the Psobioteq multicenter cohort of adults with moderate-to-severe psoriasis receiving systemic treatment. We described switches between biologics with chronograms, Sankey and Sunburst diagrams, assessed cumulative incidence of first switch by competing risks survival analysis and reasons for switching. We assessed the factors associated with the type of switch (intra-class - i.e. within the same therapeutic class - vs. inter-class) in patients switching from a TNF-alpha inhibitor using multivariate logistic regression.
A total of 2153 patients was included. The cumulative incidence of switches from first biologic was 34% at 3 years. Adalimumab and ustekinumab were the most prescribed biologic agents as first and second lines of treatment. The main reason for switching was loss of efficacy (72%), followed by adverse events (11%). Patients receiving a TNF-alpha inhibitor before 2016 mostly switched to ustekinumab, whereas those switching in 2016 or after mostly switched to an IL-17 inhibitor. Patients switching from a first-line TNF-alpha inhibitor before 2016 were more likely to switch to another TNF-alpha inhibitor compared with patients switching since 2018. Patients switching from etanercept were more likely to receive another TNF-alpha inhibitor rather than another therapeutic class of bDMARD compared with patients switching from adalimumab.
This study described the switching patterns of biologic treatments and showed how they changed over time, due to the availability of the new biologic agents primarily IL-17 inhibitors.
生物制剂是治疗中重度斑块型银屑病患者的基石,为了随着时间的推移保持临床改善,生物制剂之间的转换常常是必要的。
本研究的主要目的是准确描述生物制剂之间的转换,并随着新型生物制剂的出现,描述其随时间变化的模式。
我们纳入了在接受系统治疗的中重度银屑病成人的 Psobioteq 多中心队列中接受首次生物制剂治疗的患者。我们使用时间图表、Sankey 和 Sunburst 图描述生物制剂之间的转换,使用竞争风险生存分析评估首次转换的累积发生率和转换原因。我们评估了在从 TNF-α 抑制剂转换的患者中,与转换类型(同一治疗类别内——即同一治疗类别内——与跨类别)相关的因素,使用多变量逻辑回归。
共纳入 2153 例患者。首次生物制剂转换的累积发生率为 3 年时的 34%。阿达木单抗和乌司奴单抗是作为一线和二线治疗最常开的生物制剂。转换的主要原因是疗效丧失(72%),其次是不良事件(11%)。2016 年前接受 TNF-α 抑制剂治疗的患者大多转换为乌司奴单抗,而 2016 年或之后转换的患者大多转换为 IL-17 抑制剂。2016 年前接受一线 TNF-α 抑制剂治疗的患者比 2018 年以后接受 TNF-α 抑制剂治疗的患者更有可能转换为另一种 TNF-α 抑制剂。与从阿达木单抗转换的患者相比,从依那西普转换的患者更有可能接受另一种 TNF-α 抑制剂,而不是另一种生物制剂。
本研究描述了生物治疗的转换模式,并显示了由于新型生物制剂(主要是 IL-17 抑制剂)的出现,它们如何随时间变化。