Maternal Fetal Division, Department of Obstetrics and Gynaecology, Faculty of Medicine, Universitas Indonesia, Dr. Cipto Mangunkusumo Hospital, Jakarta, Indonesia.
Department of Obstetrics and Gynaecology, Faculty of Medicine, Universitas Indonesia, Dr. Cipto Mangunkusumo Hospital, Jakarta, Indonesia.
Womens Health (Lond). 2022 Jan-Dec;18:17455057221111066. doi: 10.1177/17455057221111066.
Although vitamin D is widely known as an essential micronutrient during pregnancy, the exact supplementation dose to prevent maternal-fetal outcomes remains a question. This study aims to provide a systematic review and a meta-analysis of data from randomized controlled trial on > 2000 IU/day vitamin D supplementation compared to ⩽ 2000 IU/day; and ⩽ 2000 IU/day compared to placebo, on their effects on the incidence of preeclampsia, gestational diabetes mellitus, preterm birth, and differences on birth weight.
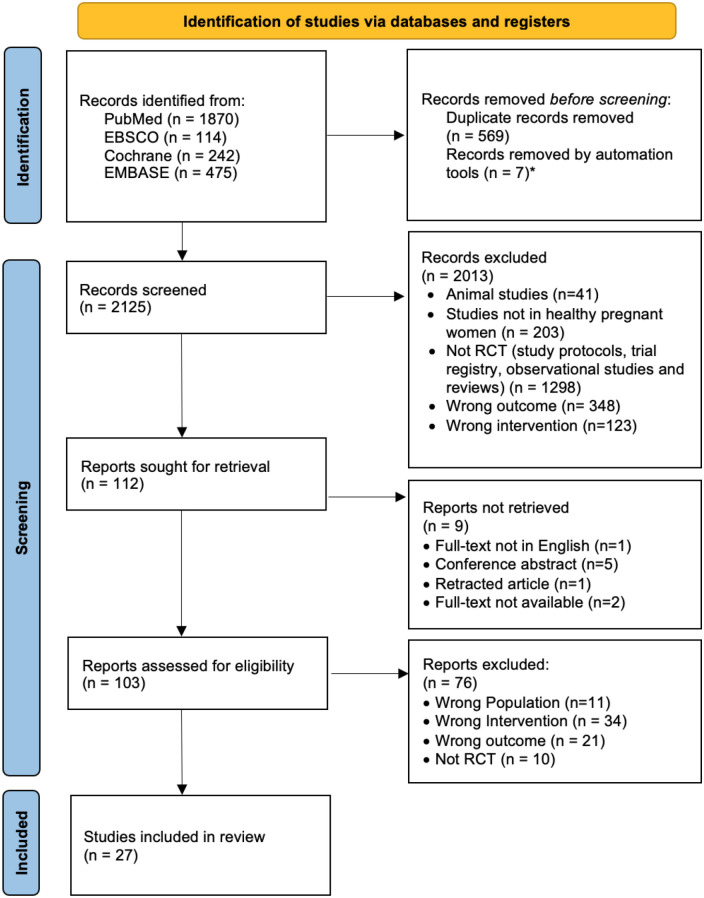
A systematic literature search on PubMed, EBSCO-MEDLINE, EMBASE, and Cochrane Central Register of Controlled Trials databases was carried out to evaluate randomized controlled trial studies on the effects of oral vitamin D > 2000 IU/day versus ⩽ 2000 IU/day; and ⩽ 2000 IU/day versus placebo, on preeclampsia, gestational diabetes mellitus, preterm birth and birth weight. Risk ratio, mean difference, and 95% confidence interval were calculated.
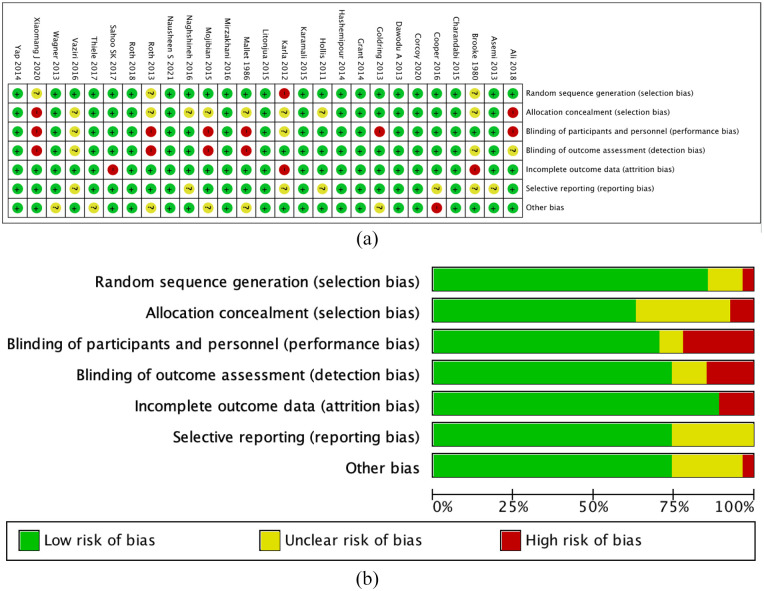
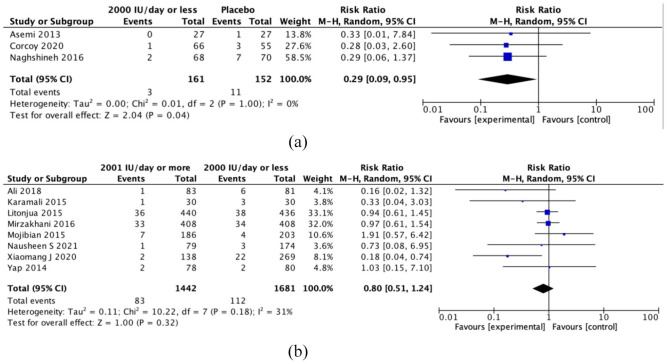
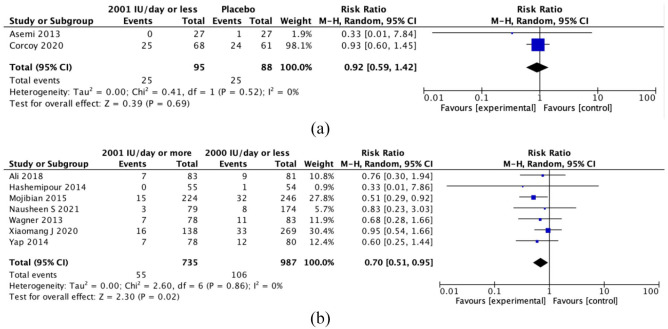
There were a total of 27 randomized controlled trials selected. Maternal vitamin D supplementation > 2000 IU/day had a positive effect only on gestational diabetes mellitus (seven randomized controlled trials; risk ratio = 0.70, 95% confidence interval: 0.51-0.95, = 0). Vitamin D supplementation ⩽ 2000 IU/day has reduced the risk of preeclampsia (three randomized controlled trials; risk ratio = 0.29, 95% confidence interval: 0.09-0.95, = 0), with no significant difference when compared to > 2000 IU/day (eight randomized controlled trials; risk ratio = 0.80, 95% confidence interval: 0.51-1.24, = 31). No difference in preterm birth risk and birth weight after vitamin D supplementation. The quality of evidence varies from moderate to very low certainty. The risk of preeclampsia and gestational diabetes mellitus after high-dose versus low-dose vitamin D supplementation was the ones with moderate certainty.
Vitamin D supplementation > 2000 IU/day might be important to reduce the risk of gestational diabetes mellitus. Lower dose vitamin D supplementation (⩽ 2000 IU/day) seemed adequate to reduce the risk of preeclampsia, with no significant difference compared to the higher dose.
尽管维生素 D 被广泛认为是妊娠期间的一种必需微量营养素,但预防母婴结局的确切补充剂量仍是一个问题。本研究旨在对超过 2000 IU/天的维生素 D 补充剂与 ⩽2000 IU/天的补充剂进行系统评价和荟萃分析;以及 ⩽2000 IU/天的补充剂与安慰剂相比,对先兆子痫、妊娠期糖尿病、早产和出生体重的影响。
对 PubMed、EBSCO-MEDLINE、EMBASE 和 Cochrane 对照试验中心注册数据库进行系统文献检索,以评估口服维生素 D ⁇ 2000 IU/天与 ⁇ 2000 IU/天;以及 ⁇ 2000 IU/天与安慰剂相比,对先兆子痫、妊娠期糖尿病、早产和出生体重的影响。计算风险比、均数差和 95%置信区间。
共选择了 27 项随机对照试验。母亲维生素 D 补充 ⁇ 2000 IU/天仅对妊娠期糖尿病有积极影响(7 项随机对照试验;风险比 ⁇ =0.70,95%置信区间:0.51-0.95, ⁇ =0)。维生素 D ⁇ 2000 IU/天的补充降低了先兆子痫的风险(3 项随机对照试验;风险比 ⁇ =0.29,95%置信区间:0.09-0.95, ⁇ =0),与 ⁇ 2000 IU/天相比无显著差异(8 项随机对照试验;风险比 ⁇ =0.80,95%置信区间:0.51-1.24, ⁇ =31)。维生素 D 补充后早产风险和出生体重无差异。证据质量从中等到极低。高剂量与低剂量维生素 D 补充后先兆子痫和妊娠期糖尿病的风险是中等确定性的。
维生素 D ⁇ 2000 IU/天以上的补充可能对降低妊娠期糖尿病的风险很重要。低剂量维生素 D 补充( ⁇ 2000 IU/天)似乎足以降低先兆子痫的风险,与高剂量相比无显著差异。