Department of Clinical Sciences, Lund University, Lund, Sweden
Department of Clinical Sciences, Helsingborg Hospital, Helsingborg, Sweden.
BMJ. 2022 Jul 12;378:e069620. doi: 10.1136/bmj-2021-069620.
To investigate the effects of fever therapy compared with no fever therapy in a wide population of febrile adults.
Systematic review with meta-analyses and trial sequential analyses of randomised clinical trials.
CENTRAL, BIOSIS, CINAHL, MEDLINE, Embase, LILACS, Scopus, and Web of Science Core Collection, searched from their inception to 2 July 2021.
Randomised clinical trials in adults diagnosed as having fever of any origin. Included experimental interventions were any fever therapy, and the control intervention had to be no fever therapy (with or without placebo/sham).
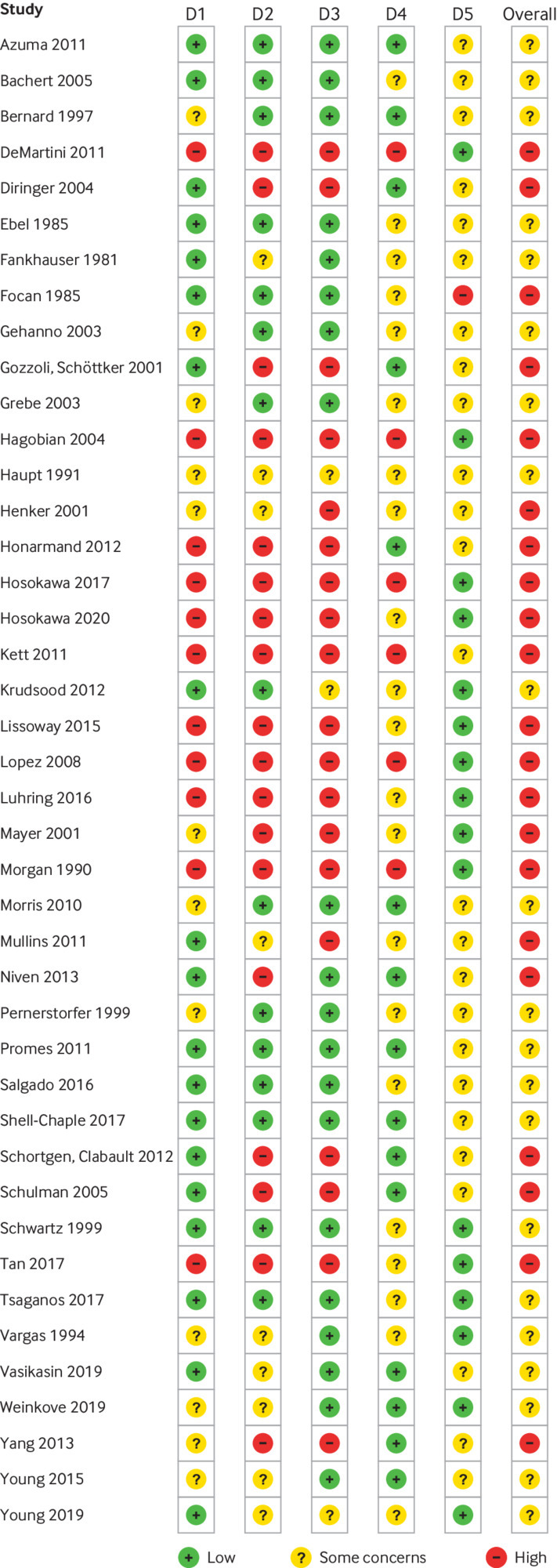
Two authors independently selected studies, extracted data, and assessed the risk of bias. Primary outcomes were all cause mortality and serious adverse events. Secondary outcomes were quality of life and non-serious adverse events. Aggregate data were synthesised with meta-analyses, subgroup analyses, and trial sequential analyses, and the evidence was assessed using the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach.
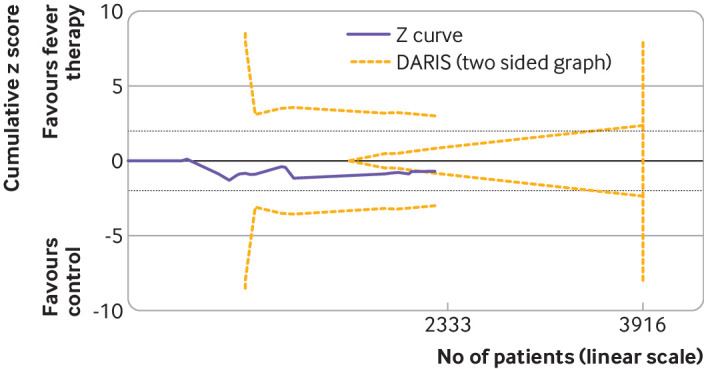
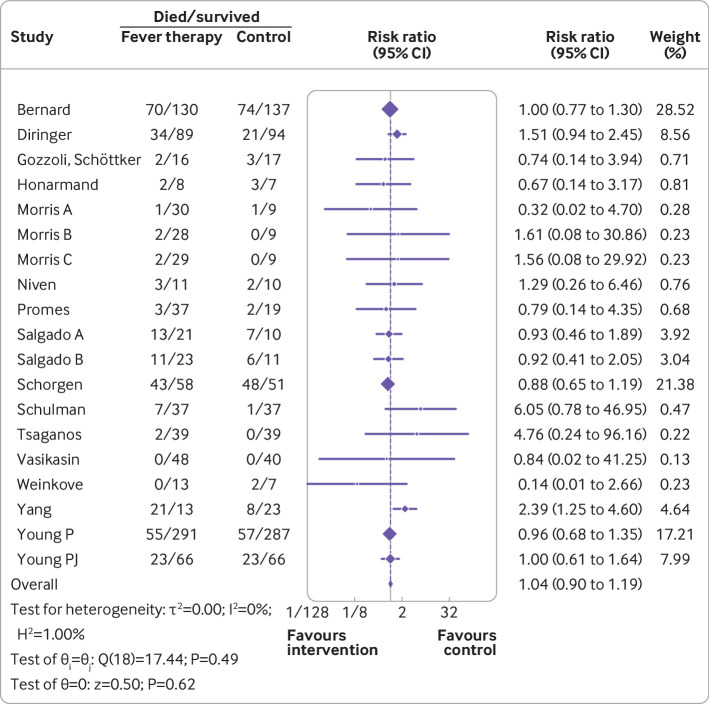
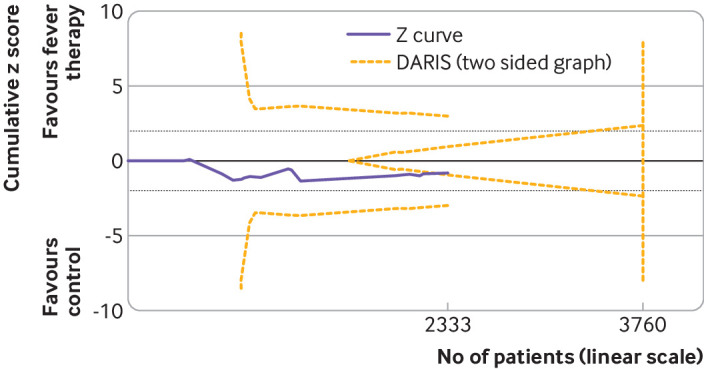
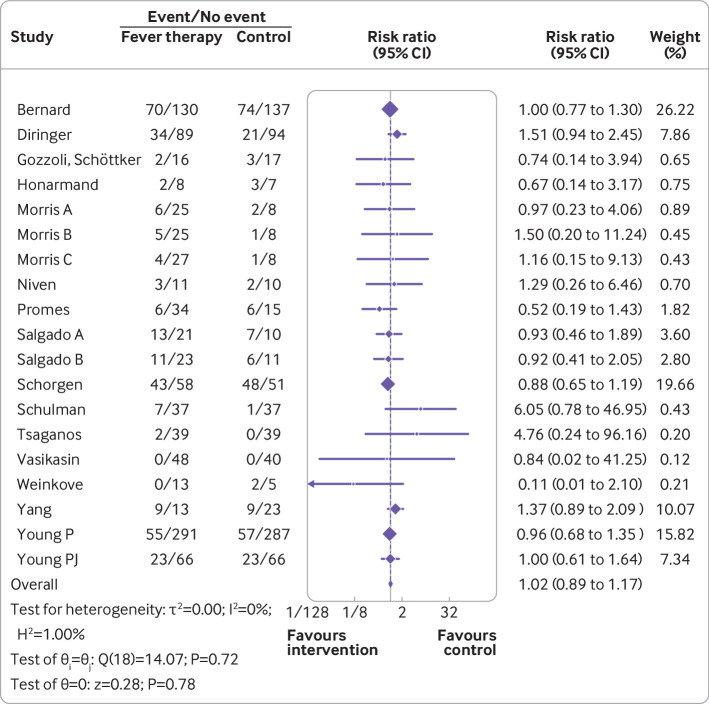
Forty two trials assessing 5140 participants were included. Twenty three trials assessed 11 different antipyretic drugs, 11 trials assessed physical cooling, and eight trials assessed a combination of antipyretic drugs and physical cooling. Of the participants, 3007 were critically ill, 1892 were non-critically ill, 3277 had infectious fever, and 1139 had non-infectious fever. All trials were assessed as being at high risk of bias. Meta-analysis and trial sequential analysis showed that the hypothesis that fever therapy reduces the risk of death (risk ratio 1.04, 95% confidence interval 0.90 to 1.19; I=0%; P=0.62; 16 trials; high certainty evidence) and the risk of serious adverse events (risk ratio 1.02, 0.89 to 1.17; I=0%; P=0.78; 16 trials; high certainty evidence) could be rejected. One trial assessing quality of life was included, showing no difference between fever therapy and control. Meta-analysis and trial sequential analysis showed that the hypothesis that fever therapy reduces the risk of non-serious adverse events could be neither confirmed nor rejected (risk ratio 0.92, 0.67 to 1.25; I=66.5%; P=0.58; four trials; very low certainty evidence).
Fever therapy does not seem to affect the risk of death and serious adverse events.
PROSPERO CRD42019134006.
在广泛的发热成人人群中,调查发热治疗与不发热治疗的效果。
对随机临床试验进行系统评价和荟萃分析及试验序贯分析。
CENTRAL、BIOSIS、CINAHL、MEDLINE、Embase、LILACS、Scopus 和 Web of Science 核心合集,从其创建到 2021 年 7 月 2 日进行搜索。
诊断为发热(病因不明)的成人的随机临床试验。纳入的实验干预措施为任何发热治疗,对照干预措施必须为不发热治疗(有无安慰剂/假治疗)。
两名作者独立选择研究、提取数据并评估偏倚风险。主要结局为全因死亡率和严重不良事件。次要结局为生活质量和非严重不良事件。使用荟萃分析、亚组分析和试验序贯分析综合汇总数据,并使用推荐、评估、制定和评估(GRADE)方法评估证据。
纳入了 42 项评估 5140 名参与者的试验。23 项试验评估了 11 种不同的退热药物,11 项试验评估了物理降温,8 项试验评估了退热药物和物理降温的联合治疗。参与者中,3007 人患有危重病,1892 人患有非危重病,3277 人患有感染性发热,1139 人患有非感染性发热。所有试验均被评估为具有高偏倚风险。荟萃分析和试验序贯分析表明,发热治疗降低死亡率风险(风险比 1.04,95%置信区间 0.90 至 1.19;I=0%;P=0.62;16 项试验;高质量证据)和严重不良事件风险(风险比 1.02,0.89 至 1.17;I=0%;P=0.78;16 项试验;高质量证据)的假设可以被拒绝。纳入了一项评估生活质量的试验,结果显示发热治疗与对照组之间无差异。荟萃分析和试验序贯分析表明,发热治疗降低非严重不良事件风险的假设既不能被证实也不能被拒绝(风险比 0.92,0.67 至 1.25;I=66.5%;P=0.58;4 项试验;极低质量证据)。
发热治疗似乎不会影响死亡和严重不良事件的风险。
PROSPERO CRD42019134006。