Hashemian Amir Masoud, Baghshani Zahra, Farzaneh Roohie, Zamani Moghadam Hamid, Maleki Fatemeh, Bagherian Farhad, Ahmadnezhad Somayyeh, Foroughian Mahdi
Department of Emergency Medicine, Faculty of Medicine, Mashhad University of Medical Sciences, Mashhad, Iran.
Department of Emergency Medicine, Mashhad University of Medical Sciences, Mashhad, Iran.
Front Med (Lausanne). 2022 Jun 29;9:872725. doi: 10.3389/fmed.2022.872725. eCollection 2022.
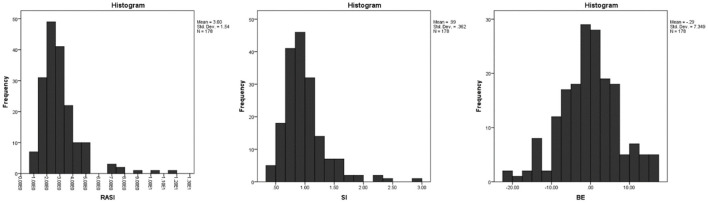
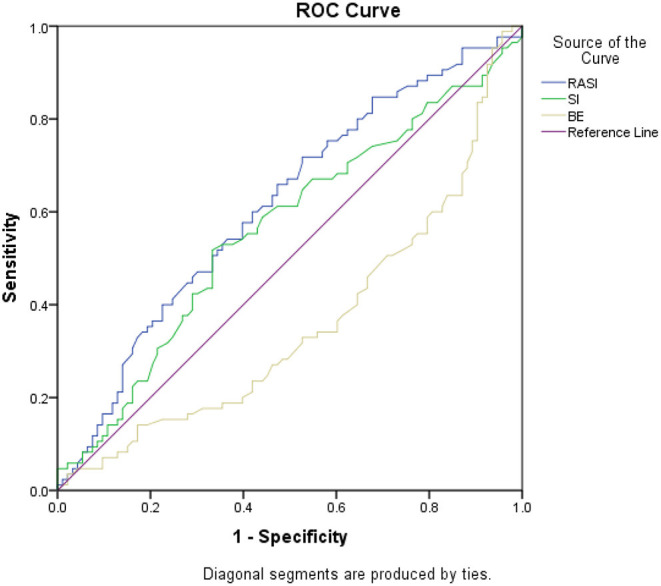
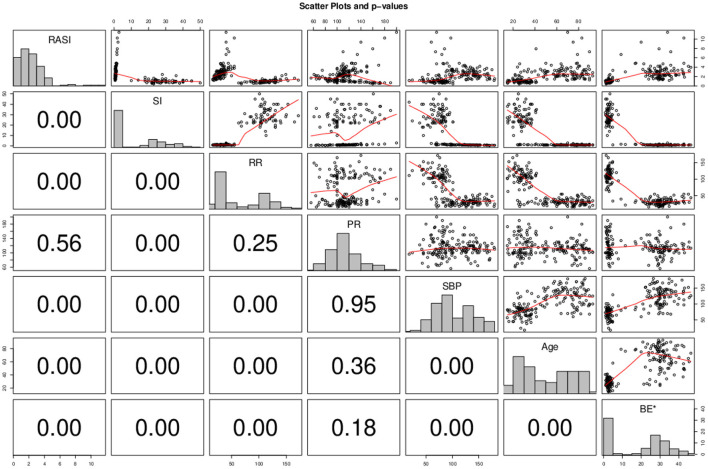
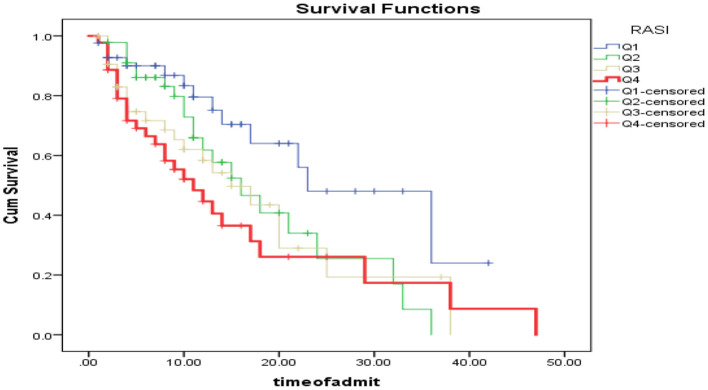
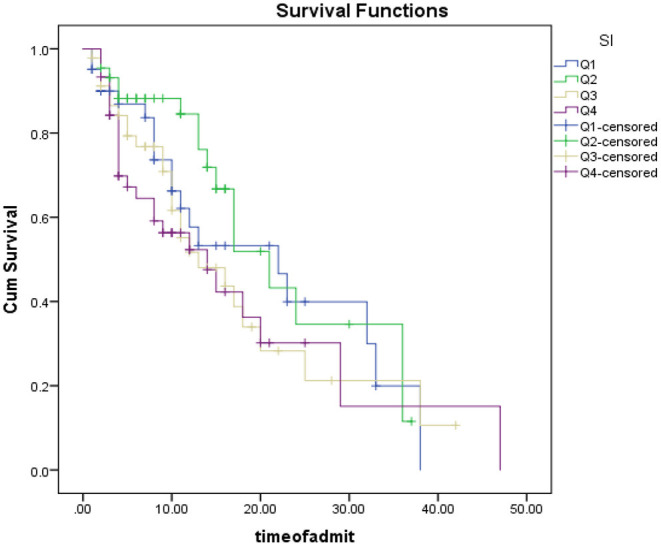
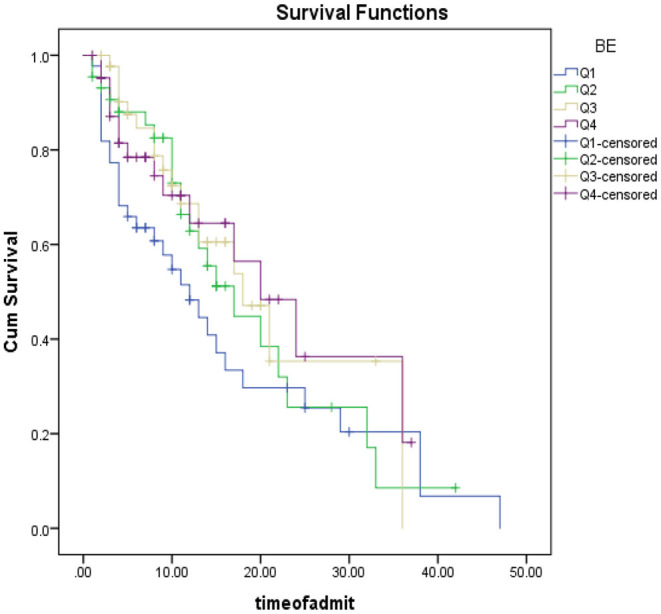
The aim of this study was to compare the relationship between shock index (SI) and respiratory adjusted shock index (RASI) scores with the final outcome of sepsis patients referred to the emergency department. This was prospective research that examined individuals who had been diagnosed with sepsis, determined by the presence of at least two of the three quick sepsis-related organ failure assessment (qSOFA) criteria and the presence of an infectious disease based on a diagnosis made by a hospital physician of Imam Reza and Ghaemshahr of Mashhad in 2019. Demographic information of patients, SI score, RASI score, and information related to the patient's clinical symptoms were recorded in the checklist. The final outcome of this study was considered mortality. Data analysis was performed using descriptive and inferential tests. In the present study, a total of 178 patients, 46 patients (25.8%) were transferred to the intensive care unit, and 98 patients (55.1%) were admitted to the normal wards. Eighty-five patients (47.75%) died and the mean length of hospital stay of all patients was 11.07 ± 9.23 days. Forty-four patients (24.7%) had referred with a decreased level of consciousness and 44 patients (24.7%) presented with confusion. The rest of the patients reported normal levels of consciousness. Kaplan Mir analysis with log-rank was performed to determine the difference in survival distribution in different SI groups: Survival distribution was not statistically different for the four defined groups (based on statistical quartiles ( = 0.320). Receiver operator curves were considered as the date of death in the case of the deceased and the date of discharge from the hospital in the case of the living as censored. The AUC of the RASI scoring system for predicting mortality was 0.614 ( = 0.009) while this value was not significant for SI ( = 0.152). In logistic regression analysis, it was found that by adjusting for the variables of age, sex, sepsis etiology, blood pressure and heart rate, level of consciousness, and gender, patients with the lower respiratory rate (OR 1.6, z = -0.159 = 0.007), younger age (OR 1.6, z = -0.029 = 0.006) and higher RASI score are more in risk of mortality (OR 1.29, z = 1.209, = 0.031). The results of our study showed that RASI scoring can be a good criterion for predicting the chance of mortality in patients with sepsis and could be used complementary to previous criteria such as SI. Patients with high RASI scores should be given more attention to reducing the chance of death.
本研究的目的是比较休克指数(SI)和呼吸调整休克指数(RASI)评分与转诊至急诊科的脓毒症患者最终结局之间的关系。这是一项前瞻性研究,研究对象为已被诊断为脓毒症的个体,其诊断依据是快速脓毒症相关器官功能衰竭评估(qSOFA)三项标准中至少两项的存在,以及基于2019年马什哈德伊玛目礼萨医院和加姆沙赫尔医院医生诊断的传染病的存在。患者的人口统计学信息、SI评分、RASI评分以及与患者临床症状相关的信息均记录在检查表中。本研究的最终结局为死亡率。数据分析采用描述性和推断性检验。在本研究中,共有178例患者,46例患者(25.8%)被转入重症监护病房,98例患者(55.1%)被收治到普通病房。85例患者(47.75%)死亡,所有患者的平均住院时间为11.07±9.23天。44例患者(24.7%)因意识水平下降前来就诊,44例患者(24.7%)表现为意识模糊。其余患者报告意识水平正常。采用对数秩的Kaplan Mir分析来确定不同SI组生存分布的差异:四个定义组(基于统计四分位数)的生存分布无统计学差异(P = 0.320)。将死亡患者的死亡日期视为删失值,存活患者的出院日期视为删失值,绘制受试者工作特征曲线。RASI评分系统预测死亡率的AUC为0.614(P = 0.009),而SI的该值无统计学意义(P = 0.152)。在逻辑回归分析中发现,在调整年龄、性别、脓毒症病因、血压和心率、意识水平及性别的变量后,呼吸频率较低的患者(OR 1.6,z = -0.159,P = 0.007)、年龄较小的患者(OR 1.6,z = -0.029,P = 0.006)以及RASI评分较高的患者死亡风险更高(OR 1.29,z = 1.209,P = 0.031)。我们的研究结果表明,RASI评分可以作为预测脓毒症患者死亡几率的良好标准,并且可以与之前的标准如SI互补使用。应更加关注RASI评分高的患者,以降低死亡几率。