Department of International Health, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland, USA.
Projahnmo Research Foundation, Dhaka, Bangladesh.
J Glob Health. 2022 Jul 23;12:05030. doi: 10.7189/jogh.12.05030.
Bangladesh reported its first COVID-19 case on March 8, 2020. Despite lockdowns and promoting behavioural interventions, as of December 31, 2021, Bangladesh reported 1.5 million confirmed cases and 27 904 COVID-19-related deaths. To understand the course of the pandemic and identify risk factors for SARs-Cov-2 infection, we conducted a cohort study from November 2020 to December 2021 in rural Bangladesh.
After obtaining informed consent and collecting baseline data on COVID-19 knowledge, comorbidities, socioeconomic status, and lifestyle, we collected data on COVID-like illness and care-seeking weekly for 54 weeks for women (n = 2683) and their children (n = 2433). Between March and July 2021, we tested all participants for SARS-CoV-2 antibodies using ROCHE's Elecsys® test kit. We calculated seropositivity rates and 95% confidence intervals (95% CI) separately for women and children. In addition, we calculated unadjusted and adjusted relative risk (RR) and 95% CI of seropositivity for different age and risk groups using log-binomial regression models.
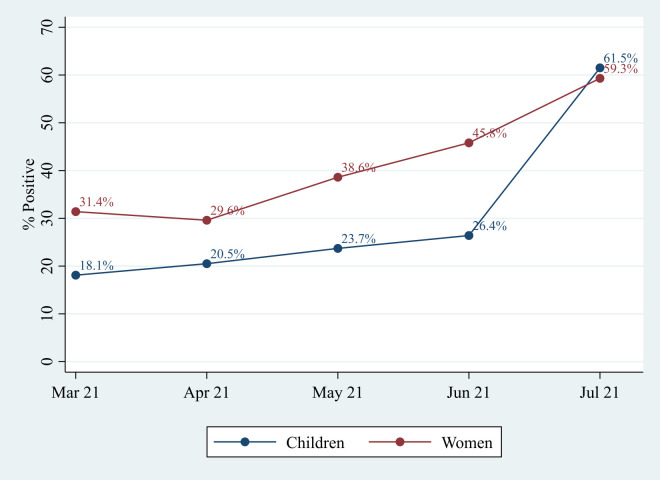
Overall, about one-third of women (35.8%, 95% CI = 33.7-37.9) and one-fifth of children (21.3%, 95% CI = 19.2-23.6) were seropositive for SARS-CoV-2 antibodies. The seroprevalence rate doubled for women and tripled for children between March 2021 and July 2021. Compared to women and children with the highest household wealth (HHW) tertile, both women and children from poorer households had a lower risk of infection (RR, 95% CI for lowest HHW tertile women (0.83 (0.71-0.97)) and children (0.75 (0.57-0.98)). Most infections were asymptomatic or mild. In addition, the risk of infection among women was higher if she reported chewing tobacco (RR = 1.19,95% CI = 1.03-1.38) and if her husband had an occupation requiring him to work indoors (RR = 1.16, 95% CI = 1.02-1.32). The risk of infection was higher among children if paternal education was >5 years (RR = 1.37, 95% CI = 1.10-1.71) than in children with a paternal education of ≤5 years.
We provided prospectively collected population-based data, which could contribute to designing feasible strategies against COVID-19 tailored to high-risk groups. The most feasible strategy may be promoting preventive care practices; however, collecting data on reported practices is inadequate. More in-depth understanding of the factors related to adoption and adherence to the practices is essential.
孟加拉国于 2020 年 3 月 8 日报告了首例 COVID-19 病例。尽管采取了封锁措施和推广行为干预措施,但截至 2021 年 12 月 31 日,孟加拉国报告了 150 万例确诊病例和 27904 例与 COVID-19 相关的死亡病例。为了了解大流行的进程并确定与 SARS-CoV-2 感染相关的风险因素,我们在孟加拉国农村地区进行了一项从 2020 年 11 月至 2021 年 12 月的队列研究。
在获得知情同意并收集有关 COVID-19 知识、合并症、社会经济状况和生活方式的基线数据后,我们每周为女性(n=2683)及其子女(n=2433)收集 54 周的 COVID 样疾病和寻求护理的数据。在 2021 年 3 月至 7 月期间,我们使用罗氏的 Elecsys®试剂盒对所有参与者进行了 SARS-CoV-2 抗体检测。我们分别为女性和儿童计算了血清阳性率和 95%置信区间(95%CI)。此外,我们使用对数二项式回归模型计算了不同年龄和风险组血清阳性的未调整和调整相对风险(RR)和 95%CI。
总体而言,约三分之一的女性(35.8%,95%CI=33.7-37.9)和五分之一的儿童(21.3%,95%CI=19.2-23.6)对 SARS-CoV-2 抗体呈血清阳性。女性的血清阳性率在 2021 年 3 月至 7 月期间翻了一番,儿童的血清阳性率翻了两番。与拥有最高家庭财富(HHW)三分位数的女性和儿童相比,来自较贫困家庭的女性和儿童感染的风险较低(HHW 最低三分位数女性(0.83(0.71-0.97))和儿童(0.75(0.57-0.98))。大多数感染是无症状或轻度的。此外,如果女性报告咀嚼烟草(RR=1.19,95%CI=1.03-1.38)或其丈夫从事需要在室内工作的职业(RR=1.16,95%CI=1.02-1.32),则她感染的风险更高。如果父亲的教育程度>5 年(RR=1.37,95%CI=1.10-1.71),则儿童感染的风险高于父亲的教育程度为≤5 年的儿童。
我们提供了前瞻性收集的基于人群的数据,这有助于针对高风险人群制定针对 COVID-19 的可行策略。最可行的策略可能是促进预防保健措施;然而,收集有关报告做法的数据是不够的。更深入地了解与采用和坚持这些实践相关的因素至关重要。