Infectious Diseases Division (IDD), International Centre for Diarrhoeal Disease Research, Dhaka, Bangladesh
Infectious Diseases Division (IDD), International Centre for Diarrhoeal Disease Research, Dhaka, Bangladesh.
BMJ Open. 2021 Dec 2;11(12):e055169. doi: 10.1136/bmjopen-2021-055169.
To establish a hospital-based platform to explore the epidemiological and clinical characteristics of patients screened for COVID-19.
Hospital-based surveillance.
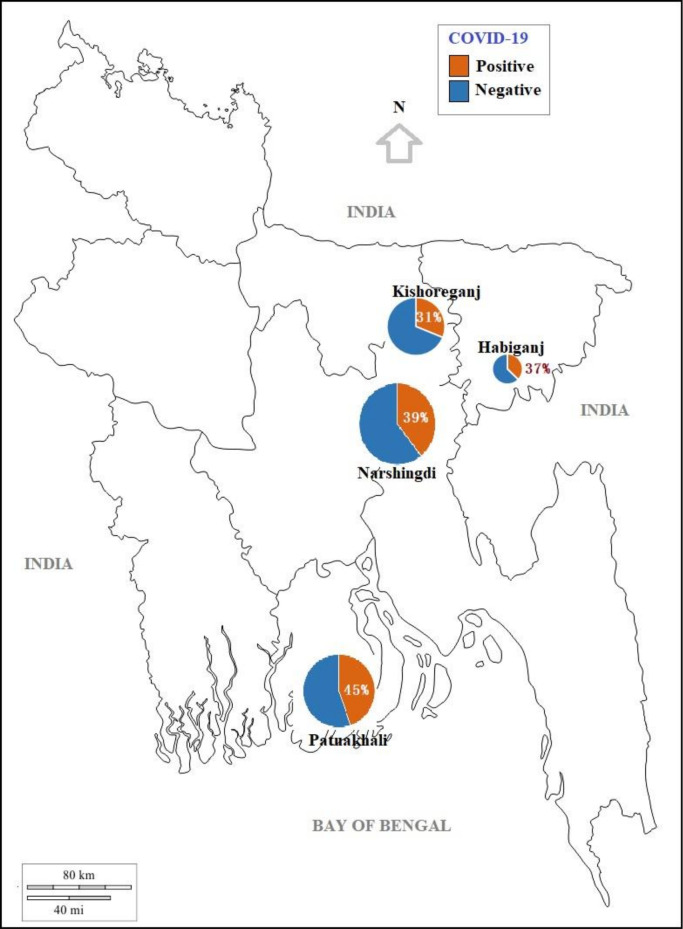
This study was conducted in four selected hospitals in Bangladesh during 10 June-31 August 2020.
In total, 2345 patients of all age (68% male) attending the outpatient and inpatient departments of surveillance hospitals with any one or more of the following symptoms within last 7 days: fever, cough, sore throat and respiratory distress.
The outcome measures were COVID-19 positivity and mortality rate among enrolled patients. Pearson's χ test was used to compare the categorical variables (sign/symptoms, comorbidities, admission status and COVID-19 test results). Regression analysis was performed to determine the association between potential risk factors and death.
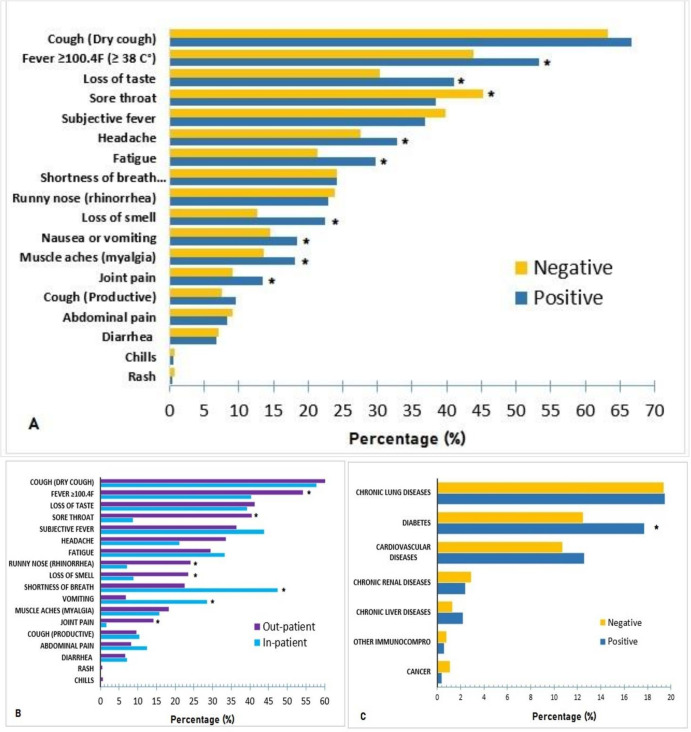
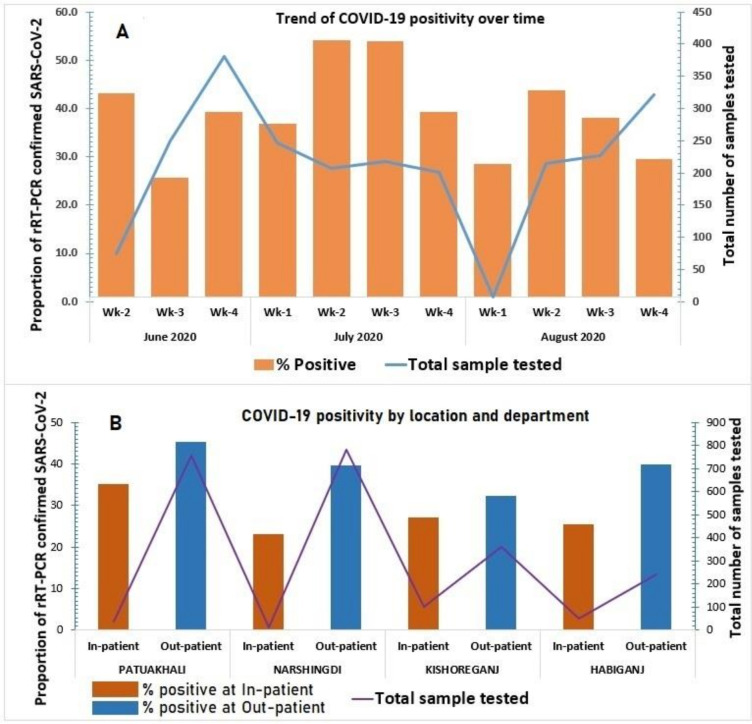
COVID-19 was detected among 922 (39%) enrolled patients. It was more common in outpatients with a peak positivity in second week of July (112, 54%). The median age of the confirmed COVID-19 cases was 38 years (IQR: 30-50), 654 (71%) were male and 83 (9%) were healthcare workers. Cough (615, 67%) was the most common symptom, followed by fever (493, 53%). Patients with diabetes were more likely to get COVID-19 than patients without diabetes (48% vs 38%; OR: 1.5; 95% CI: 1.2 to 1.9). The death rate among COVID-19 positive was 2.3%, n=21. Death was associated with age ≥60 years (adjusted OR (AOR): 13.9; 95% CI: 5.5 to 34), shortness of breath (AOR: 9.7; 95% CI: 3.0 to 30), comorbidity (AOR: 4.8; 95% CI: 1.1 to 21.7), smoking history (AOR: 2.2, 95% CI: 0.7 to 7.1), attending the hospital in <2 days of symptom onset due to critical illness (AOR: 4.7; 95% CI: 1.2 to 17.8) and hospital admission (AOR: 3.4; 95% CI: 1.2 to 9.8).
COVID-19 positivity was observed in more than one-third of patients with suspected COVID-19 attending selected hospitals. While managing such patients, the risk factors identified for higher death rates should be considered.
建立一个基于医院的平台,以探索筛查 COVID-19 的患者的流行病学和临床特征。
基于医院的监测。
本研究于 2020 年 6 月 10 日至 8 月 31 日在孟加拉国的四家选定医院进行。
共有 2345 名年龄在 68%为男性的患者,他们在过去 7 天内出现以下任何一种或多种症状:发热、咳嗽、喉咙痛和呼吸窘迫,在监测医院的门诊和住院部门就诊。
结局指标为登记患者的 COVID-19 阳性率和死亡率。采用 Pearson χ 检验比较分类变量(体征/症状、合并症、入院状态和 COVID-19 检测结果)。采用回归分析确定潜在危险因素与死亡之间的关系。
在登记的 2345 名患者中,有 922 名(39%)患者检测出 COVID-19 阳性。门诊患者中 COVID-19 阳性率更高,7 月第二周达到峰值(112 例,54%)。确诊 COVID-19 病例的中位年龄为 38 岁(IQR:30-50),654 例(71%)为男性,83 例(9%)为医务人员。咳嗽(615 例,67%)是最常见的症状,其次是发热(493 例,53%)。患有糖尿病的患者比没有糖尿病的患者更有可能感染 COVID-19(48%比 38%;OR:1.5;95%CI:1.2 至 1.9)。COVID-19 阳性患者的死亡率为 2.3%,n=21。死亡与年龄≥60 岁(调整后的 OR(AOR):13.9;95%CI:5.5 至 34)、呼吸急促(AOR:9.7;95%CI:3.0 至 30)、合并症(AOR:4.8;95%CI:1.1 至 21.7)、吸烟史(AOR:2.2,95%CI:0.7 至 7.1)、因病情严重在症状出现后 2 天内就诊于医院(AOR:4.7;95%CI:1.2 至 17.8)和住院(AOR:3.4;95%CI:1.2 至 9.8)有关。
在接受选定医院治疗的疑似 COVID-19 患者中,有超过三分之一的患者 COVID-19 检测呈阳性。在治疗这些患者时,应考虑与较高死亡率相关的已确定危险因素。