Vaccine Alliance Aotearoa New Zealand and Malaghan Institute of Medical Research, PO Box 7060, Wellington 6242, New Zealand.
Pacific Clinical Research Network, 1289 Haupapa St, Rotorua 3010, New Zealand.
Vaccine. 2022 Aug 12;40(34):5050-5059. doi: 10.1016/j.vaccine.2022.07.009. Epub 2022 Jul 12.
There is very little known about SARS-CoV-2 vaccine immune responses in New Zealand populations at greatest risk for serious COVID-19 disease.
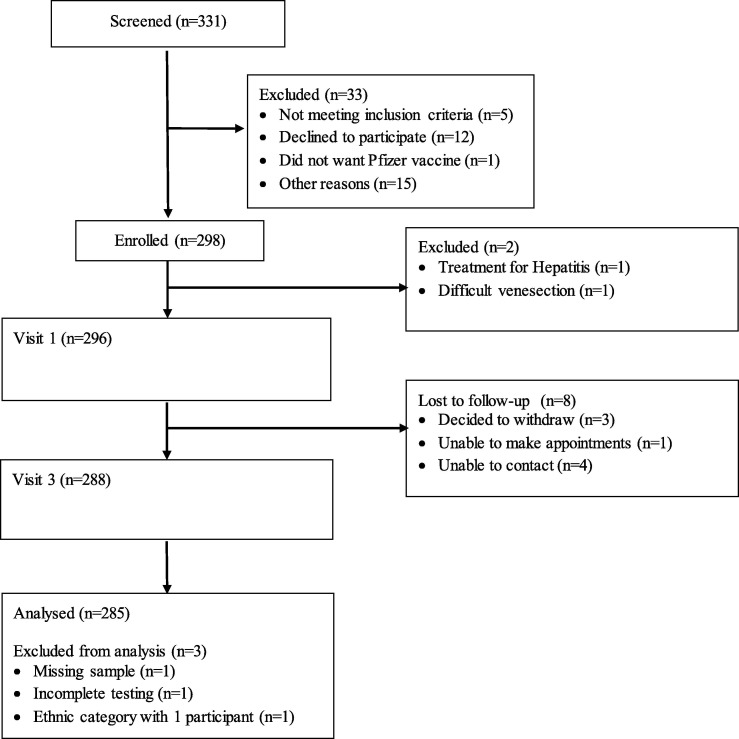
This prospective cohort study assessed immunogenicity in BNT162b2 mRNA vaccine recipients in New Zealand without previous COVID-19, with enrichment for Māori, Pacific peoples, older adults ≥ 65 years of age, and those with co-morbidities. Serum samples were analysed at baseline and 28 days after second dose for presence of quantitative anti-S IgG by chemiluminescent microparticle immunoassay and for neutralizing capacity against Wuhan, Beta, Delta, and Omicron BA.1 strains using a surrogate viral neutralisation assay.
285 adults with median age of 52 years were included. 55% were female, 30% were Māori, 28% were Pacific peoples, and 26% were ≥ 65 years of age. Obesity, cardiac and pulmonary disease and diabetes were more common than in the general population. All participants received 2 doses of BNT162b2 vaccine. At 28 days after second vaccination, 99.6% seroconverted to the vaccine, and anti-S IgG and neutralising antibody levels were high across gender and ethnic groups. IgG and neutralising responses declined with age. Lower responses were associated with age ≥ 75 and diabetes, but not BMI. The ability to neutralise the Omicron BA.1 variant in vitro was severely diminished but maintained against other variants of concern.
Vaccine antibody responses to BNT162b2 were generally robust and consistent with international data in this COVID-19 naïve cohort with representation of key populations at risk for COVID-19 morbidity. Subsequent data on response to boosters, durability of responses and cellular immune responses should be assessed with attention to elderly adults and diabetics.
对于新西兰患严重 COVID-19 疾病风险最高的人群,有关 SARS-CoV-2 疫苗免疫反应的信息知之甚少。
本前瞻性队列研究评估了在新西兰未感染过 COVID-19 的 BNT162b2 mRNA 疫苗接种者的免疫原性,其中包括毛利人、太平洋岛民、≥65 岁的老年人以及患有合并症的人群。在第 2 剂后 28 天,通过化学发光微粒子免疫测定分析血清样本中定量抗-S IgG 的存在情况,并使用替代病毒中和测定分析针对武汉、Beta、Delta 和 Omicron BA.1 株的中和能力。
共纳入 285 名中位年龄为 52 岁的成年人。55%为女性,30%为毛利人,28%为太平洋岛民,26%为≥65 岁。肥胖、心脏和肺部疾病以及糖尿病比一般人群更为常见。所有参与者均接受了 2 剂 BNT162b2 疫苗接种。在第 2 剂后 28 天,99.6%的人血清转化为疫苗,并且在性别和种族群体中,抗-S IgG 和中和抗体水平均很高。随着年龄的增长,IgG 和中和抗体的反应下降。年龄≥75 岁和患有糖尿病与较低的反应相关,但与 BMI 无关。体外中和奥密克戎 BA.1 变异株的能力严重减弱,但对其他关注变异株的中和能力得以维持。
在这个 COVID-19 初发队列中,BNT162b2 的疫苗抗体反应通常是强大且一致的,该队列中代表性关键人群为 COVID-19 发病风险较高的人群。应评估后续关于加强针的反应、反应的持久性和细胞免疫反应的数据,特别关注老年人群和糖尿病患者。