Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, New York.
Department of Surgery, Memorial Sloan Kettering Cancer Center, New York, New York.
JAMA Netw Open. 2022 Jul 1;5(7):e2224296. doi: 10.1001/jamanetworkopen.2022.24296.
The COVID-19 pandemic led to disruptions in delivery of cancer treatments; factors associated with treatment delay among patients with cancer who contract COVID-19 need further characterization.
To assess the associations of patient factors, social determinants of health, severity of COVID-19, and timing of COVID-19 diagnosis with the risk of treatment delay.
DESIGN, SETTING, AND PARTICIPANTS: This prospective cohort study was conducted from March 2020 through July 2021 at 60 academic and community medical practices in the United States. Participants included patients with any cancer diagnosis who were scheduled for treatment and contracted COVID-19. Data were analyzed in February 2022.
Positive test result for SARS-CoV-2.
The main outcomes were treatment delay, defined as more than 14 days between the date originally planned for treatment and the date of initiation of therapy, or discontinuation of therapy. Multivariable analyses were used to assess outcomes.
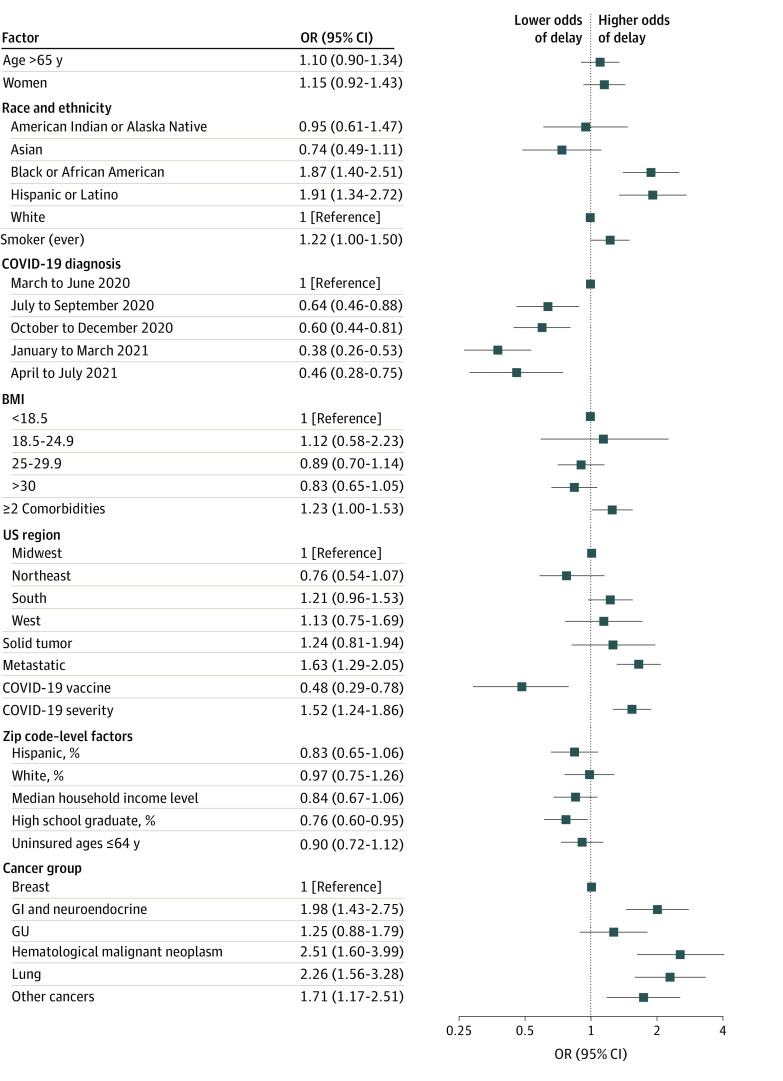
A total of 3028 patients (1470 patients [49%] aged ≥65 years; 1741 [58%] women) were included in the registry. With 962 of 2103 patients (46%) experiencing anticancer drug delay or discontinuation, delays were higher among Black patients compared with White patients (odds ratio [OR], 1.87; 95% CI, 1.40-2.51), Hispanic or Latino patients compared with non-Hispanic or Latino patients (OR, 1.91; 95% CI, 1.34-2.72), patients with 2 or more comorbidities compared with patients with 0 to 1 (OR, 1.23; 95% CI, 1.00-1.53), patients with metastatic disease rather than locoregional disease (OR, 1.63; 95% CI, 1.29-2.05), and patients who experienced COVID-19 complications compared with those who did not (OR, 1.52; 95% CI, 1.24-1.86). Residing in an area with a higher proportion of residents reporting Hispanic or Latino ethnicity (OR, 0.76; 95% CI, 0.60-0.95) and contracting COVID-19 later in the pandemic, compared with those who were infected in March to June 2020, (eg, January to March 2021: OR, 0.38; 95% CI, 0.26-0.53) were associated with lower likelihood of drug therapy delay. A total of 95 of 202 patients (47%) experienced delay or discontinuation of radiation treatment, with having 2 or more comorbidities associated with delay (OR, 2.69; 95% CI, 1.20-6.20). Higher local-area median household income was associated with lower likelihood of radiation treatment delay (OR, 0.41; 95% CI, 0.17-0.94). There were 89 of 125 patients (71%) who experienced surgical treatment delay, and delays were higher among patients in the South compared with those in the Midwest (OR, 9.66; 95% CI, 2.14-52.3). Interestingly, patients with 2 or more comorbidities, compared with those with 0 to 1, experienced lower likelihoods of surgical treatment delay (OR, 0.26; 95% CI, 0.07-0.88).
Our findings suggest that individual patient factors, social determinants of health, and COVID-19 severity and diagnosis date were associated with exacerbated health disparities during the pandemic in regards to cancer treatment delay.
COVID-19 大流行导致癌症治疗中断;需要进一步描述感染 COVID-19 的癌症患者治疗延迟的相关因素。
评估患者因素、健康社会决定因素、COVID-19 严重程度和 COVID-19 诊断时间与治疗延迟风险的相关性。
设计、地点和参与者:这是一项前瞻性队列研究,于 2020 年 3 月至 2021 年 7 月在美国 60 家学术和社区医疗实践中进行。参与者包括计划接受治疗且感染 COVID-19 的任何癌症诊断患者。数据分析于 2022 年 2 月进行。
SARS-CoV-2 检测结果呈阳性。
主要结果是治疗延迟,定义为从最初计划治疗日期到开始治疗的日期超过 14 天,或停止治疗。多变量分析用于评估结果。
共有 3028 名患者(≥65 岁患者 1470 名[49%];女性 1741 名[58%])纳入登记处。在 2103 名患者中有 962 名(46%)经历了抗癌药物延迟或停药,与白人患者相比,黑人患者的延迟率更高(比值比[OR],1.87;95%CI,1.40-2.51),西班牙裔或拉丁裔患者比非西班牙裔或拉丁裔患者更高(OR,1.91;95%CI,1.34-2.72),有 2 种或更多合并症的患者比有 0 至 1 种合并症的患者更高(OR,1.23;95%CI,1.00-1.53),转移性疾病患者比局部区域疾病患者更高(OR,1.63;95%CI,1.29-2.05),且发生 COVID-19 并发症的患者比未发生 COVID-19 并发症的患者更高(OR,1.52;95%CI,1.24-1.86)。与报告西班牙裔或拉丁裔居民比例较高的地区(OR,0.76;95%CI,0.60-0.95)和与 2020 年 3 月至 6 月(例如,2021 年 1 月至 3 月:OR,0.38;95%CI,0.26-0.53)相比,在疫情后期感染 COVID-19 的患者相比,居住在地区的患者(OR,0.38;95%CI,0.26-0.53),癌症药物治疗延迟的可能性较低。202 名患者中有 95 名(47%)经历了放射治疗的延迟或停止,其中 2 种或更多合并症与延迟相关(OR,2.69;95%CI,1.20-6.20)。较高的当地中等家庭收入与较低的放射治疗延迟可能性相关(OR,0.41;95%CI,0.17-0.94)。125 名患者中有 89 名(71%)经历了手术治疗延迟,与中西部患者相比,南部患者的延迟率更高(OR,9.66;95%CI,2.14-52.3)。有趣的是,与有 0 至 1 种合并症的患者相比,有 2 种或更多合并症的患者手术治疗延迟的可能性较低(OR,0.26;95%CI,0.07-0.88)。
我们的研究结果表明,在 COVID-19 大流行期间,个体患者因素、健康社会决定因素、COVID-19 严重程度和诊断日期与癌症治疗延迟的加剧健康差异有关。