Department of Epidemiology and Health Studies, Universidad de Los Andes, San Carlos de Apoquindo 2200, Las Condes, 7620001, Santiago, Chile.
Independent Consultant, Santiago, Chile.
BMC Public Health. 2022 Jul 29;22(1):1443. doi: 10.1186/s12889-022-13841-2.
Previous representative health surveys conducted in Chile evidenced a high obesity prevalence rate among adults, especially in female and urban areas. Nevertheless, these have limited utility for targeted interventions and local source allocation for prevention. This study analyzes the increments in obesity prevalence rates in populations ≥15 years of age and the geographic variation at the regional level. We also assessed whether the obesity rates have different patterns on a smaller geographic level than national and regional ones.
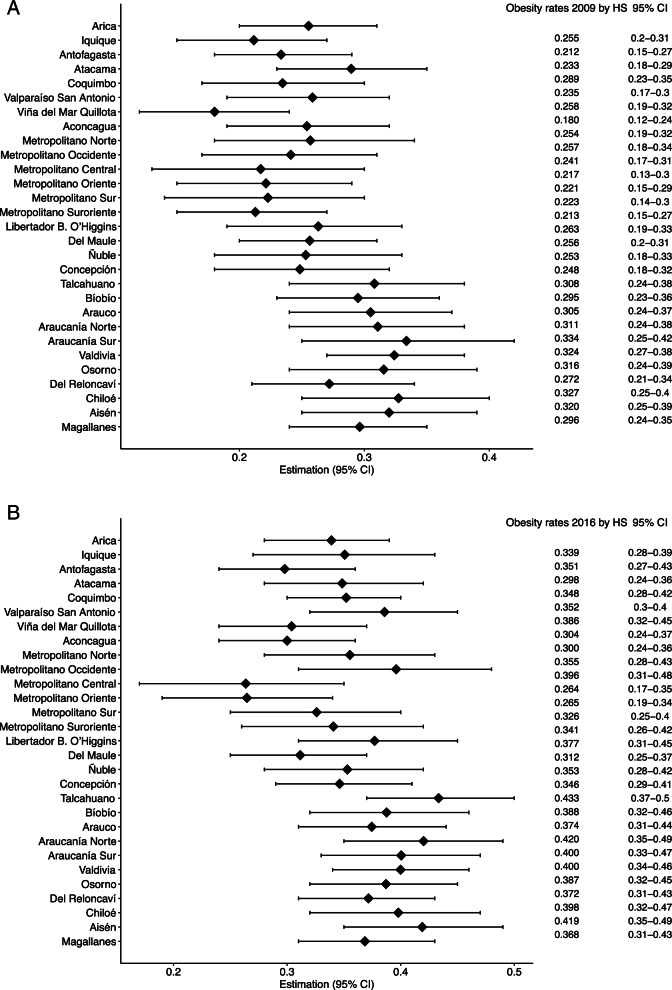
This ecological study analyzed data from two representative national samples of adolescents and adults ≥15 years old, who participated in the last Chilean health surveys, 2009 (n = 5412) and 2016 (n = 6233). Obesity (body mass index≥30 kg/m) rates were calculated on the national, regional, and Health service (HS) levels, being HS the smallest unit of analysis available. Obesity rates and relative increase to early identify target populations and geographic areas, with 95% confidence intervals (95% CI), were calculated using the sampling design of the national surveys, at the national and regional level, and by gender, age groups, and socioeconomic status. The Fay-Herriot (FH) models, using auxiliary data, were fitted for obesity rate estimates at the HS level.
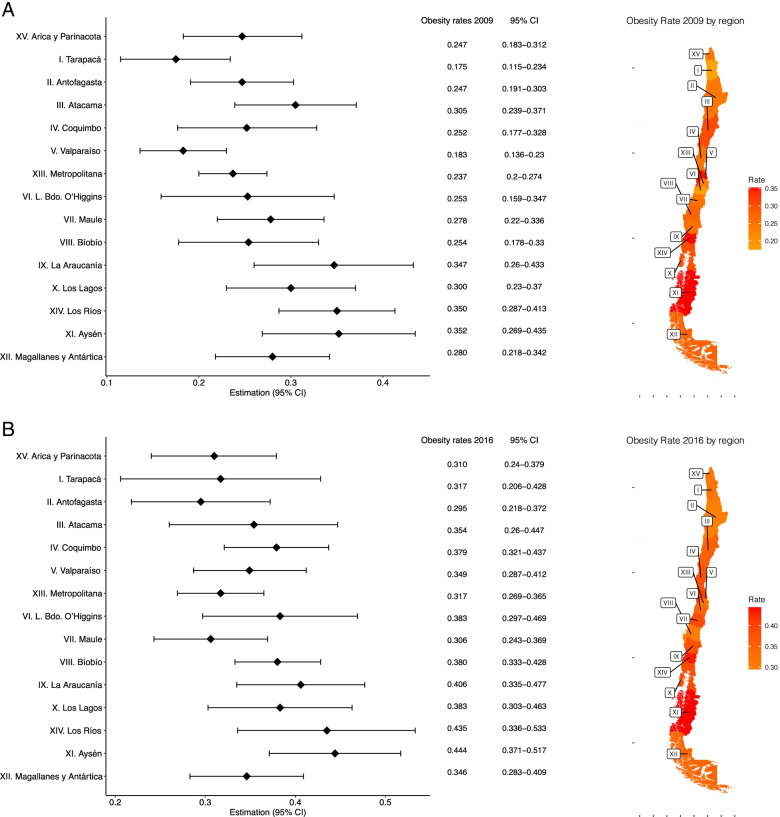
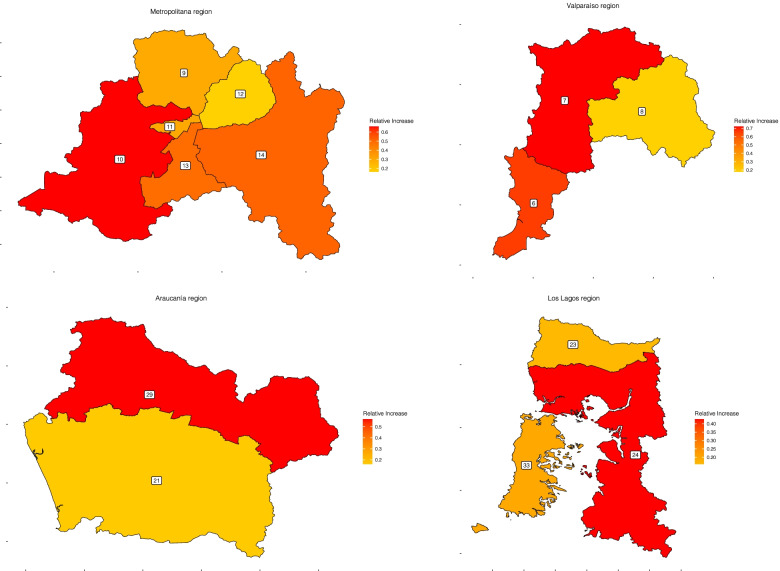
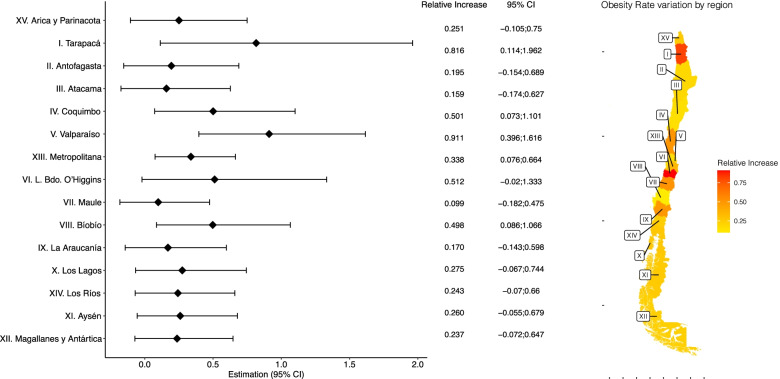
The relative increase in obesity rate was 37.1% (95%CI 23.3-52.9) at the national level, with a heterogeneous geographic distribution at the regional one. Southern regions had the highest obesity rates in both surveys (Aysén: 35.2, 95%CI 26.9-43.5 in 2009, 44.3 95%CI 37-51.7 in 2016), but higher increases were predominantly in the northern and central areas of the country (relative increase 91.1 95%CI 39.6-110.1 in Valparaiso and 81.6 95%CI 14.4-196.2 in Tarapacá). Obesity rates were higher in females, older age, and lower socioeconomic groups; nevertheless, relative increases were higher in the opposite ones. The FH estimates showed an obesity rates variation at the HS level, where higher rates tend to converge to specific HS areas of each region.
Obesity rates and relative increase are diverse across subnational levels and substantially differ from the national estimates, highlighting a pattern that converges to areas with low-middle income households. Our results emphasize geographical disparities in obesity prevalence among adults and adolescents.
智利之前进行的具有代表性的健康调查表明,成年人,尤其是女性和城市地区的肥胖患病率很高。然而,这些调查对于有针对性的干预措施和预防的当地资源分配的作用有限。本研究分析了≥15 岁人群肥胖患病率的增长情况以及区域层面的地理差异。我们还评估了肥胖率在较小的地理层面(比国家和地区层面)是否具有不同的模式。
这项生态研究分析了参加最近两次智利健康调查的两个具有代表性的青少年和≥15 岁成年人的全国样本数据,分别为 2009 年(n=5412)和 2016 年(n=6233)。在国家、地区和卫生服务(HS)层面计算肥胖(身体质量指数≥30kg/m)率,HS 是可分析的最小单位。使用全国调查的抽样设计,在国家和地区层面以及按性别、年龄组和社会经济地位计算肥胖率和相对增长率,以早期确定目标人群和地理区域,置信区间为 95%(95%CI)。使用辅助数据拟合 Fay-Herriot(FH)模型,以估算 HS 层面的肥胖率。
肥胖率的相对增长率为 37.1%(95%CI 23.3-52.9),在区域层面上呈异质地理分布。南部地区在这两项调查中肥胖率最高(2009 年阿伊森大区为 35.2,95%CI 26.9-43.5,2016 年为 44.3,95%CI 37-51.7),但增长幅度主要集中在该国北部和中部地区(瓦尔帕莱索大区的相对增长率为 91.1,95%CI 39.6-110.1,塔拉帕卡大区为 81.6,95%CI 14.4-196.2)。女性、年龄较大和社会经济地位较低的人群肥胖率较高;然而,相对增长率较高的是相反的人群。FH 估计显示 HS 层面的肥胖率存在差异,其中高肥胖率趋于集中在每个地区特定的 HS 区域。
肥胖率和相对增长率在次国家层面上存在差异,与国家估计值有很大不同,突出了一种向中低收入家庭集中的模式。我们的研究结果强调了成年人和青少年肥胖流行率的地理差异。