Concord Hospital, Sydney, NSW.
University of Sydney, Sydney, NSW.
Med J Aust. 2022 Aug 15;217(4):212-217. doi: 10.5694/mja2.51656. Epub 2022 Jul 31.
This consensus statement of Australian clinicians provides new recommendations for the pharmacological management of heart failure based on studies reported since the publication of the 2018 Australian heart failure guidelines.
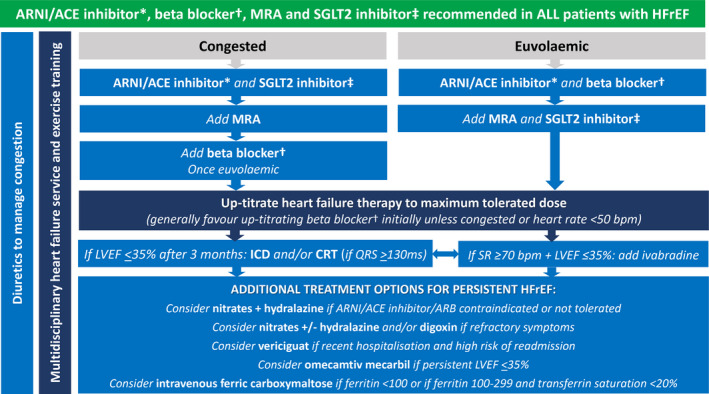
▪Use of sodium-glucose cotransporter 2 (SGLT2) inhibitors to prevent hospitalisation for heart failure in type 2 diabetes mellitus can be extended to patients with multiple cardiovascular risk factors, albuminuric chronic kidney disease, or atherosclerotic cardiovascular disease. ▪New evidence supports the use of a mineralocorticoid receptor antagonist (finerenone) to prevent heart failure in type 2 diabetes mellitus associated with albuminuric chronic kidney disease. ▪In addition to renin angiotensin system inhibitors (angiotensin receptor neprilysin inhibitor preferred), beta blockers and mineralocorticoid receptor antagonists, an SGLT2 inhibitor (dapagliflozin or empagliflozin) is recommended in all patients with heart failure with reduced left ventricular ejection fraction (LVEF ≤ 40%) (HFrEF). Lower quality evidence supports these therapies in patients with heart failure with mildly reduced LVEF (41-49%) (HFmrEF). ▪A soluble guanylate cyclase stimulator (vericiguat), selective cardiac myosin activator (omecamtiv mecarbil) and, if iron deficient, intravenous iron (ferric carboxymaltose) provide additional benefits in persistent HFrEF. ▪An SGLT2 inhibitor (empagliflozin) should be considered in patients with heart failure with preserved LVEF (≥ 50%) (HFpEF). Key changes in management from this statement: This document broadens the scope of angiotensin receptor neprilysin inhibitor use in patients with HFrEF and HFmrEF. SGLT2 inhibitor use expands to become a cornerstone therapy in HFrEF, with increasing evidence to support its use in HFmrEF and HFpEF.
这份澳大利亚临床医生的共识声明基于 2018 年澳大利亚心力衰竭指南发布以来报告的研究,为心力衰竭的药物治疗提供了新的建议。
可以将钠-葡萄糖共转运蛋白 2(SGLT2)抑制剂用于预防 2 型糖尿病患者因心力衰竭住院,扩展到具有多种心血管风险因素、白蛋白尿性慢性肾脏病或动脉粥样硬化性心血管疾病的患者。
新证据支持使用盐皮质激素受体拮抗剂(非奈利酮)预防与白蛋白尿性慢性肾脏病相关的 2 型糖尿病患者心力衰竭。
除了肾素-血管紧张素系统抑制剂(首选血管紧张素受体脑啡肽酶抑制剂)、β受体阻滞剂和盐皮质激素受体拮抗剂外,所有射血分数降低的心力衰竭(LVEF≤40%)(HFrEF)患者均推荐使用 SGLT2 抑制剂(达格列净或恩格列净)。心力衰竭伴轻度射血分数降低(41-49%)(HFmrEF)患者的这些治疗方法的证据质量较低。
可溶性鸟苷酸环化酶刺激剂(维立西呱)、选择性心肌肌球蛋白激活剂(奥马卡汀美卡比)和如果缺铁,则给予静脉铁(羧基麦芽糖铁)为持续性 HFrEF 患者提供额外获益。
射血分数保留的心力衰竭(≥50%)(HFpEF)患者应考虑使用 SGLT2 抑制剂(恩格列净)。
本文扩大了血管紧张素受体脑啡肽酶抑制剂在 HFrEF 和 HFmrEF 患者中的应用范围。SGLT2 抑制剂的使用扩展成为 HFrEF 的基石治疗方法,越来越多的证据支持其在 HFmrEF 和 HFpEF 中的应用。