Liu Xin, Guo Siyu, Xu Zhicheng
Department of Critical Care Medicine, The First Affiliated Hospital of Gannan Medical University, Ganzhou, China.
Medical Department, Queen Mary School, Nanchang University, Nanchang, China.
Front Cardiovasc Med. 2022 Jul 15;9:961000. doi: 10.3389/fcvm.2022.961000. eCollection 2022.
Intracranial hemorrhage (ICH) is excluded in most anticoagulation randomized clinical trials (RCTs), so oral anticoagulant (OAC) therapy is still the conventional treatment for patients with atrial fibrillation (AF) after ICH. Therefore, we conducted a meta-analysis to determine the effectiveness and safety outcomes of OAC for these patients.
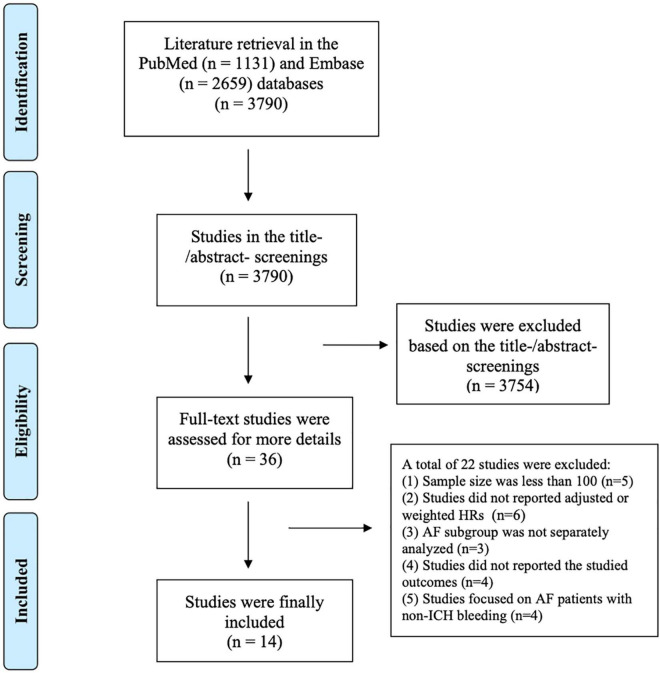
We systematically searched the PubMed and Embase databases up to March 2022 for RCTs and observational studies exploring the effect of OAC in patients with AF after ICH. The effectiveness outcomes included stroke or systemic embolism, ischemic stroke, and all-cause death, whereas the safety outcomes were major bleeding and recurrent ICH. Hazard ratios (HRs) and 95% confidence intervals (CIs) from each study were pooled using a random-effects model.
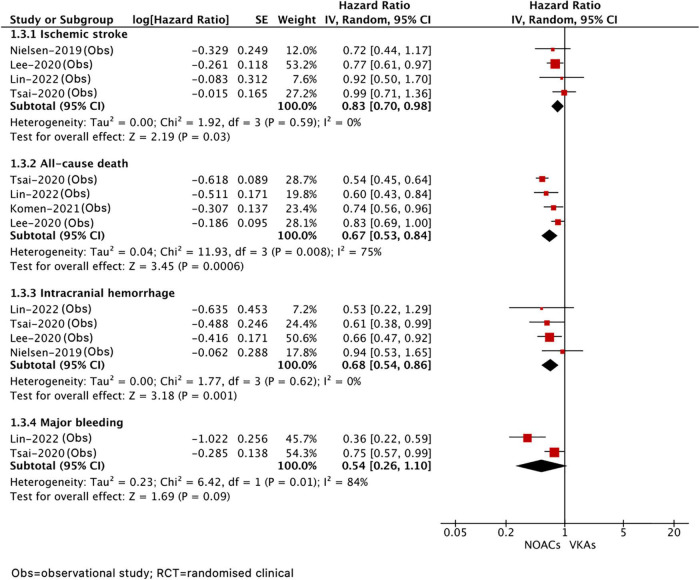
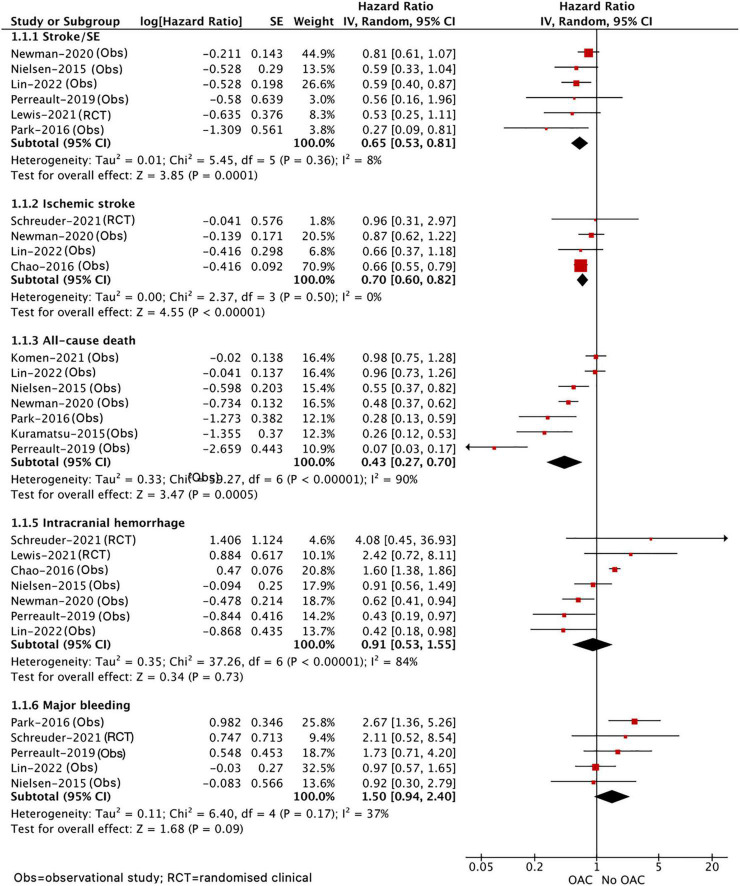
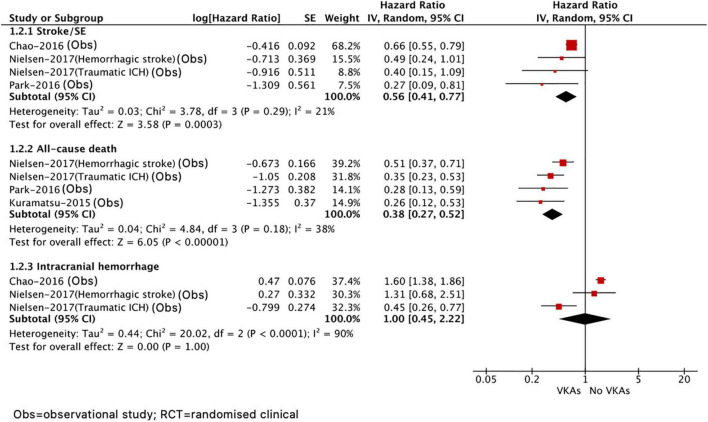
A total of 14 studies were included. The OAC therapy that was performed reduced the risks of stroke or systemic embolism (HR = 0.65, 95% CI 0.53-0.81), ischemic stroke (HR = 0.70, 95% CI 0.60-0.82), and all-cause death (HR = 0.43, 95% CI 0.27-0.70) but had a higher risk of major bleeding (HR = 1.50, 95% CI 0.94-2.40) and showed no difference in recurrent ICH (HR = 0.91, 95% CI 0.53-1.55) compared to the no OAC therapy. With the use of non-vitamin K antagonist oral anticoagulant (NOAC) therapy, a lower risk of stroke or systemic embolism (HR = 0.83, 95% CI 0.70-0.98), all-cause death (HR = 0.67, 95% CI 0.53-0.84), and recurrent ICH (HR = 0.68, 95% CI 0.54-0.86) was observed against the use of vitamin K antagonists (VKA) therapy.
The OAC therapy (especially VKA) revealed superior effectiveness in patients with AF after ICH, and the superiority of NOAC was also found, but some related evidence was limited.
大多数抗凝随机临床试验(RCT)都排除了颅内出血(ICH)患者,因此口服抗凝药(OAC)治疗仍是脑出血后房颤(AF)患者的常规治疗方法。因此,我们进行了一项荟萃分析,以确定OAC对这些患者的有效性和安全性结果。
我们系统检索了截至2022年3月的PubMed和Embase数据库,以查找探索OAC对脑出血后房颤患者影响的RCT和观察性研究。有效性结果包括中风或全身性栓塞、缺血性中风和全因死亡,而安全性结果是大出血和复发性ICH。使用随机效应模型汇总每项研究的风险比(HR)和95%置信区间(CI)。
共纳入14项研究。与未进行OAC治疗相比,进行OAC治疗可降低中风或全身性栓塞(HR = 0.65,95% CI 0.53-0.81)、缺血性中风(HR = 0.70,95% CI 0.60-0.82)和全因死亡(HR = 0.43,95% CI 0.27-0.70)的风险,但大出血风险更高(HR = 1.50,95% CI 0.94-2.40),复发性ICH无差异(HR = 0.91,95% CI 0.53-1.55)。与使用维生素K拮抗剂(VKA)治疗相比,使用非维生素K拮抗剂口服抗凝药(NOAC)治疗可降低中风或全身性栓塞(HR = 0.83,95% CI 0.70-0.98)、全因死亡(HR = 0.67,95% CI 0.53-0.84)和复发性ICH(HR = 0.68,95% CI 0.54-0.86)的风险。
OAC治疗(尤其是VKA)在脑出血后房颤患者中显示出更好的有效性,也发现了NOAC的优势,但一些相关证据有限。