Department of Radiology, Shinshu University School of Medicine, 3-1-1 Asahi, Matsumoto, 390-8621, Japan.
Jpn J Radiol. 2022 Dec;40(12):1213-1234. doi: 10.1007/s11604-022-01321-x. Epub 2022 Aug 2.
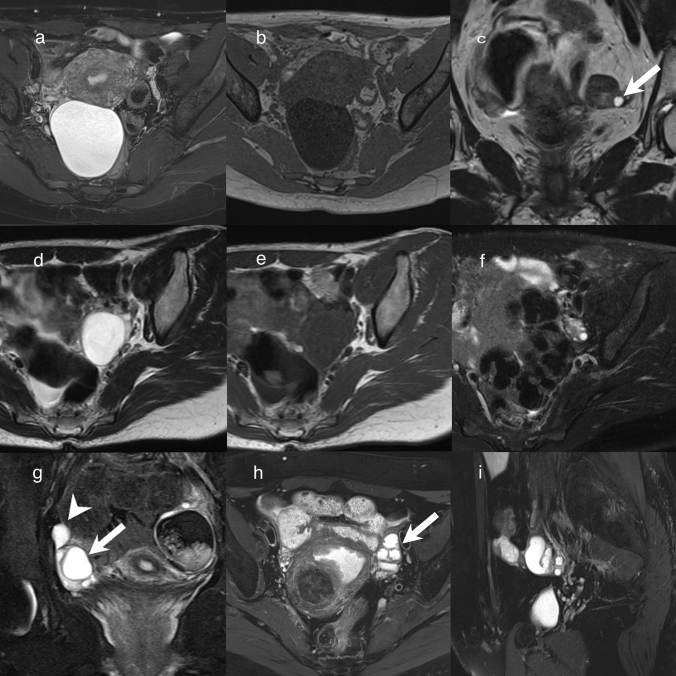
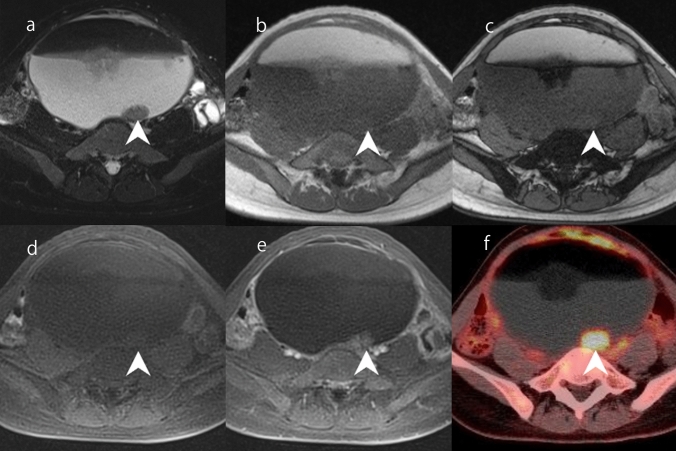
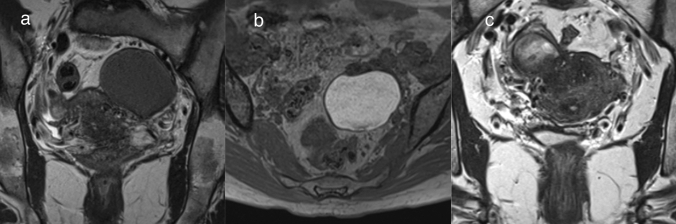
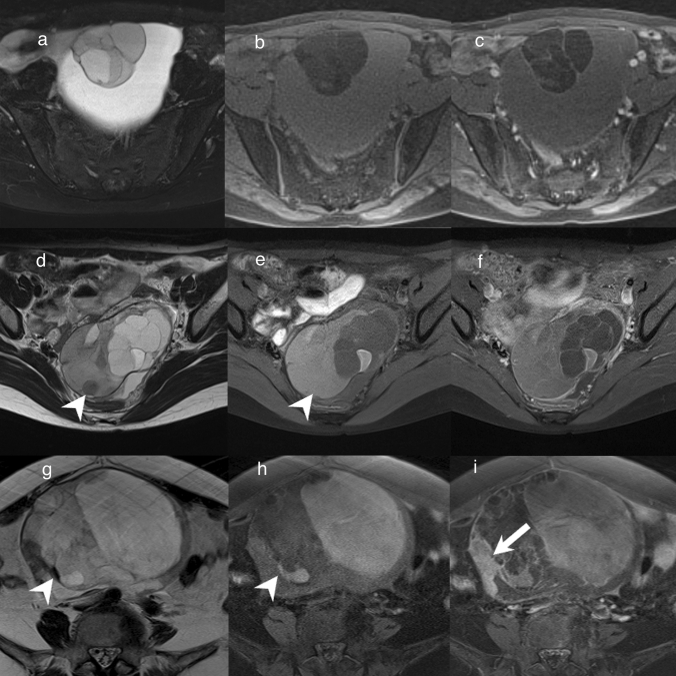
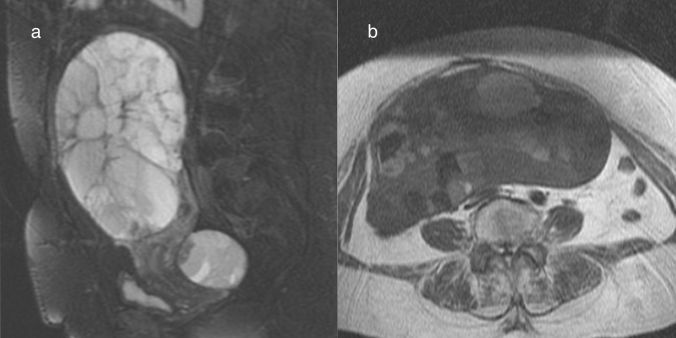
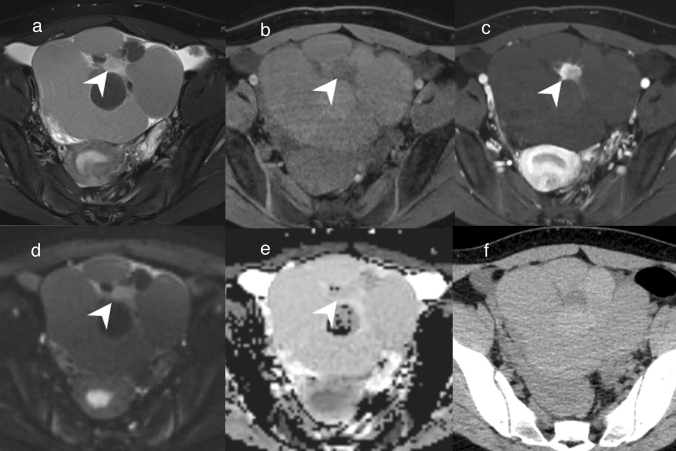
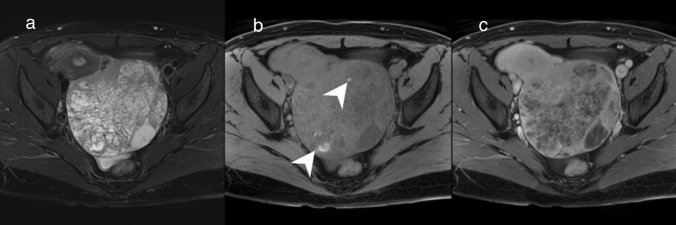
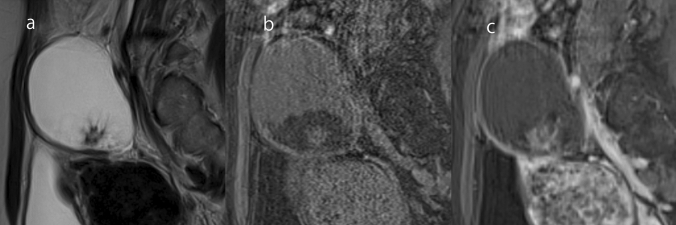
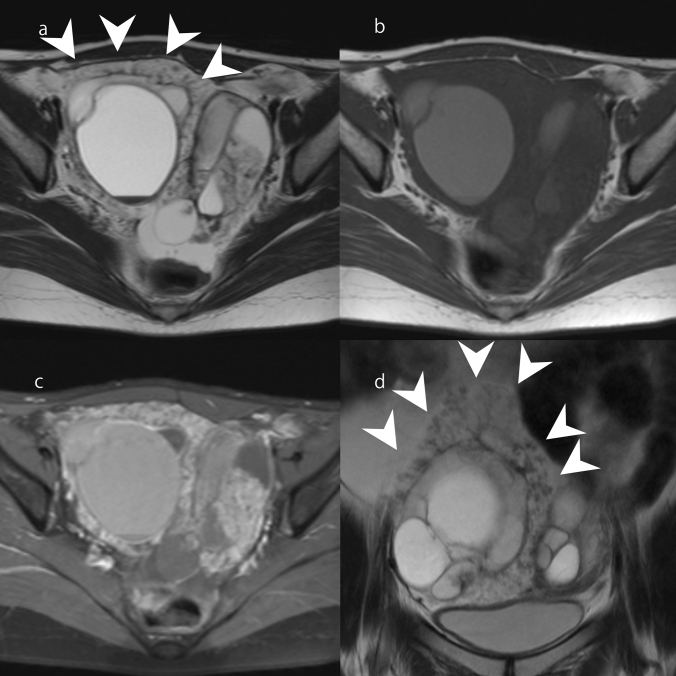
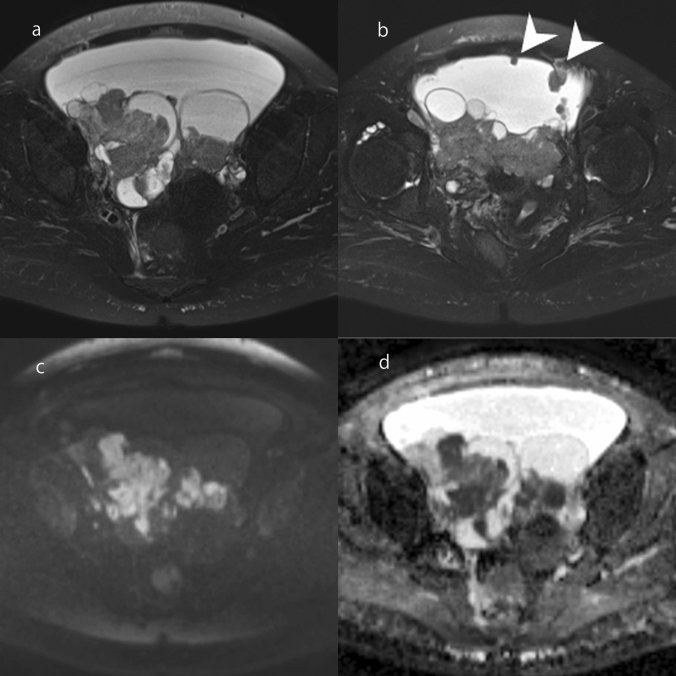
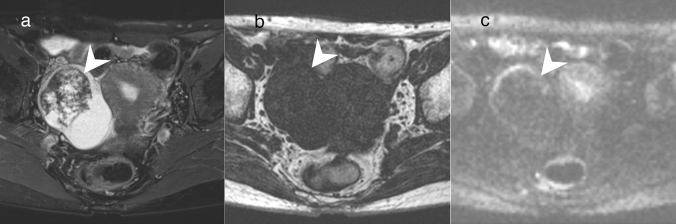
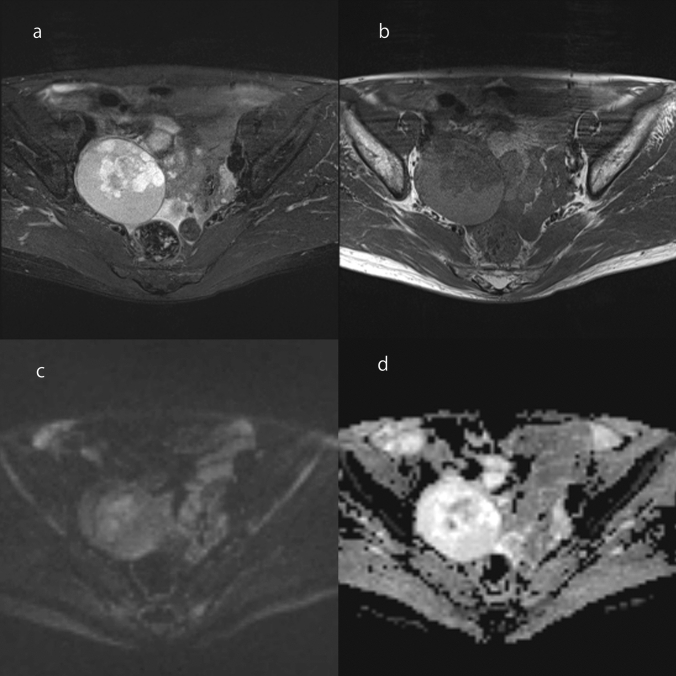
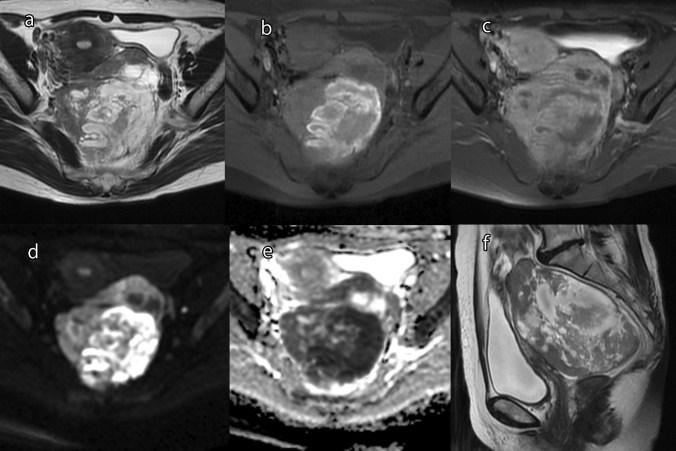
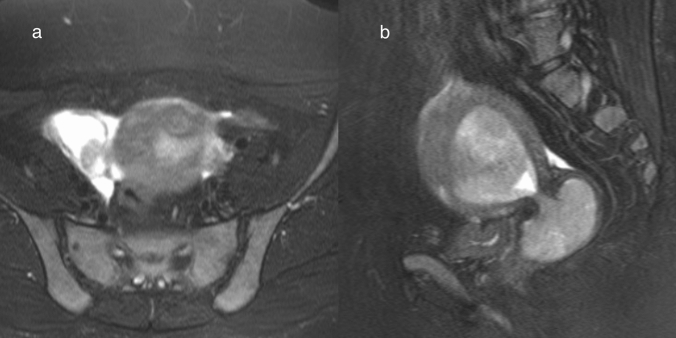
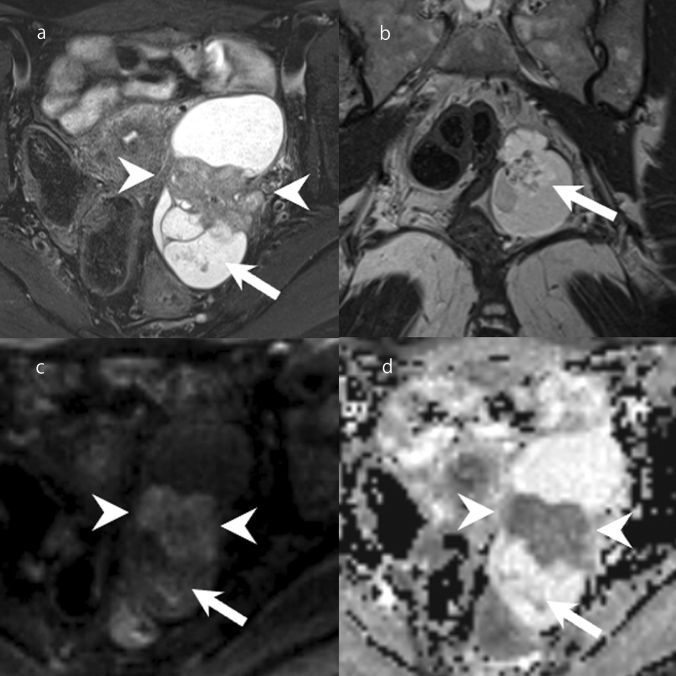
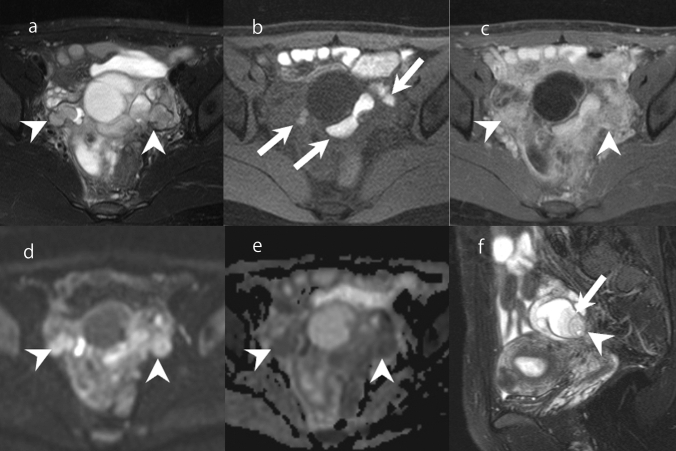
There are many types of ovarian tumors, and these different types often form cystic masses with a similar appearance, which can make their differentiation difficult. However, with the exclusion of rare ovarian tumors, the number of ovarian tumors encountered in daily practice is somewhat fixed. It goes without saying that magnetic resonance imaging (MRI) is useful for differentiating ovarian tumors. In this review, we summarize the differential diagnoses for each of the five types of MRI findings commonly encountered in daily practice. First, unilocular cystic masses without mural nodules/solid components include benign lesions such as serous cystadenoma, functional cysts, surface epithelial inclusion cysts, paratubal cysts, and endometriosis. Second, multilocular cystic ovarian lesions include mucinous tumors and ovarian metastases. It should be noted that mucinous tumors may be diagnosed as borderline or carcinoma, even if no solid component is observed. Third, cystic lesions with mural nodules that are unrelated to endometriosis include serous borderline tumor and serous carcinoma. Cystic lesions with solid components are more likely to be malignant, but some may be diagnosed as benign. Fourth, ovarian tumors deriving from endometriosis include seromucinous borderline tumors, endometrioid carcinoma, and clear cell carcinoma. These tumors sometimes need to be differentiated from serous tumors. Finally, cystic lesions with lipid contents include teratoma-related tumors. In mature cystic teratoma, mural nodules (called "Rokitansky protuberance" or "dermoid nipple") are sometimes seen, but they do not suggest malignancy. Some of these lesions can be diagnosed accurately by considering their characteristic imaging findings, their changes over time, MRI findings other than those of the primary lesion, and information from other modalities such as tumor markers. To ensure the optimal treatment for ovarian tumors, it is important to estimate the histological type as well as to diagnose whether a lesion is benign or malignant.
卵巢肿瘤有很多种类型,这些不同类型的肿瘤通常形成外观相似的囊性肿块,这使得它们的鉴别变得困难。然而,除了罕见的卵巢肿瘤外,在日常实践中遇到的卵巢肿瘤数量是相对固定的。不言而喻,磁共振成像(MRI)有助于鉴别卵巢肿瘤。在本篇综述中,我们总结了在日常实践中常见的五种 MRI 表现类型的鉴别诊断。首先,无壁结节/实性成分的单房性囊性肿块包括良性病变,如浆液性囊腺瘤、功能性囊肿、表面上皮包涵囊肿、副输卵管囊肿和子宫内膜异位症。其次,多房性囊性卵巢病变包括黏液性肿瘤和卵巢转移瘤。需要注意的是,即使没有实性成分,黏液性肿瘤也可能被诊断为交界性或癌。第三,与子宫内膜异位症无关的壁结节性囊性病变包括浆液性交界性肿瘤和浆液性癌。囊性病变伴实性成分更倾向于恶性,但有些可能被诊断为良性。第四,源于子宫内膜异位症的卵巢肿瘤包括黏液性-浆液性交界性肿瘤、子宫内膜样癌和透明细胞癌。这些肿瘤有时需要与浆液性肿瘤相鉴别。最后,含脂类物质的囊性病变包括与畸胎瘤相关的肿瘤。在成熟囊性畸胎瘤中,有时可见壁结节(称为“Rokitansky 结节”或“皮样乳头”),但这并不提示恶性。通过考虑其特征性影像学表现、随时间的变化、原发性病变以外的 MRI 表现以及肿瘤标志物等其他影像学检查的信息,可以对其中一些病变进行准确诊断。为了对卵巢肿瘤进行最佳治疗,估计组织学类型以及诊断病变是良性还是恶性是很重要的。