Department of Epidemiology and Biostatistics, School of Public Health, Peking University, Beijing, China.
National Institute for Nutrition and Health, Chinese Center for Disease Control and Prevention, Beijing, China.
Lancet Public Health. 2022 Dec;7(12):e994-e1004. doi: 10.1016/S2468-2667(22)00110-4. Epub 2022 Aug 1.
The improvement of life expectancy is one of the aims of the Healthy China 2030 blueprint. We aimed to investigate the extent to which healthy lifestyles are associated with life expectancy in Chinese adults.
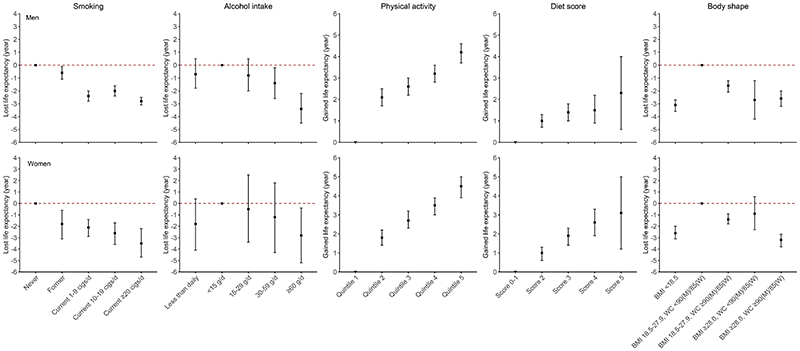
We used the prospective China Kadoorie Biobank (CKB) study to examine the relative risk of mortality associated with individual and combined lifestyle factors (never smoking or quitting not for illness, no excessive alcohol use, being physically active, healthy eating habits, and healthy body shape). Participants with coronary heart disease, stroke, cancer, or missing values for body-mass index were excluded. For analysis of chronic respiratory diseases, participants with chronic obstructive pulmonary disease or asthma were excluded. We estimated the national prevalence of lifestyle factors using data from the China Nutrition and Health Surveillance (CNHS; 2015) and derived mortality rates from the Global Burden of Diseases, Injuries, and Risk Factors Study (2015). All three data sources were combined to estimate the life expectancy of individuals at age 30 years following different levels of lifestyle factors by using the life table method. The cause-specific decomposition of the life expectancy differences was analysed using Arriaga's method.
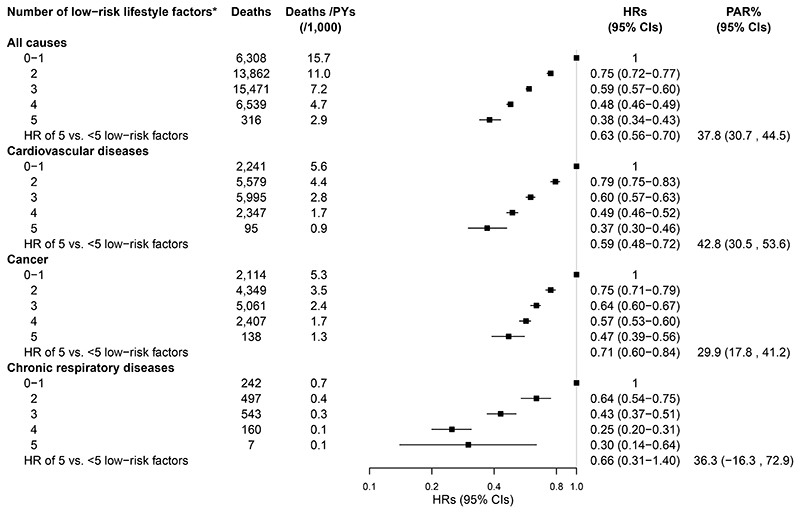
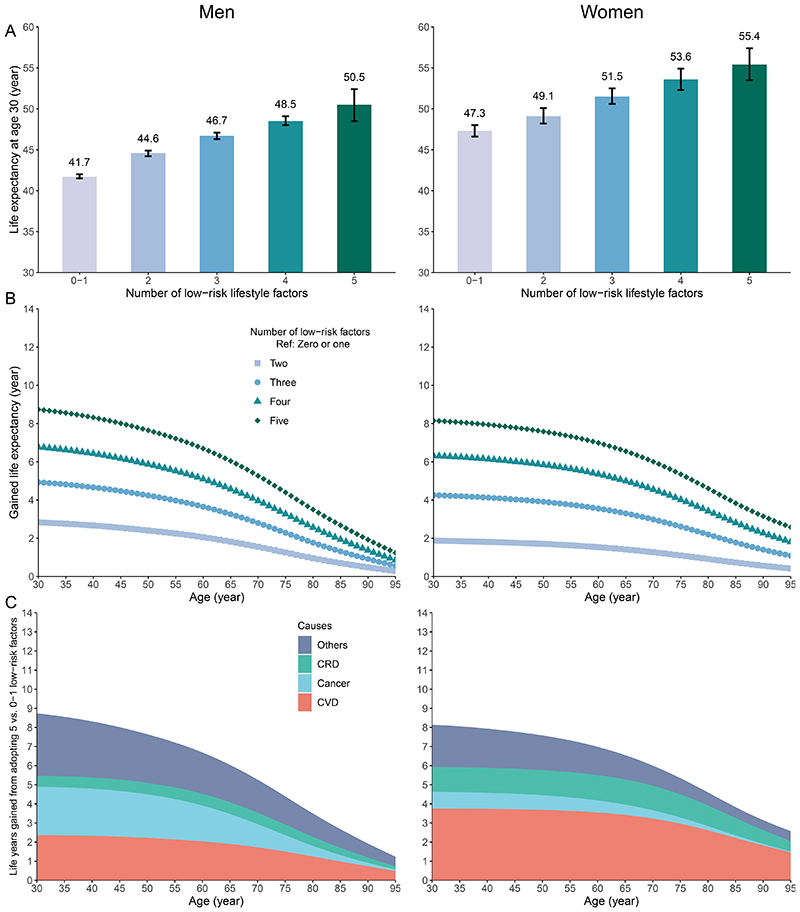
After the exclusion of CKB participants with coronary heart disease, stroke, cancer, or missing BMI data at baseline, 487 209 were included in the primary analysis. Participants with COPD or asthma at baseline were additionally excluded for chronic respiratory disease-related analysis, leaving 451 233 participants with data available for analysis. Data from 171 127 adults aged 30-84 years from the CNHS 2015 were used to estimate the sex-specific and age-specific prevalence of lifestyle-related factors. There were 42 496 deaths documented over a median follow-up of 11·1 years (IQR 10·2-12·1) in CKB. The adjusted hazard ratios (aHRs) of participants adopting five versus 0-1 low-risk factors was 0·38 (95% CI 0·34-0·43) for all-cause mortality, aHR 0·37 (0·30-0·46) for cardiovascular disease mortality, aHR 0·47 (0·39-0·56) for cancer mortality, and aHR 0·30 (0·14-0·64) for chronic respiratory disease mortality. The life expectancy at age 30 years for individuals with 0-1 low-risk factors was on average 41·7 years (95% CI 41·5-42·0) for men and 47·3 years (46·6-48·0) for women. For individuals with all five low-risk factors, the life expectancy at age 30 was 50·5 years (95% CI 48·5-52·4) for men and 55·4 years (53·5-57·4) for women; meaning a difference of 8·8 years (95% CI 6·8-10·7) for men and 8·1 years (6·5-9·9) for women. The estimated extended life expectancy for men and women was mainly attributable to reduced death from cardiovascular disease (2·4 years [27% of the total extended life expectancy] for men and 3·7 years [46%] for women), cancer (2·6 years [30%] for men and 0·9 years [11%] for women), and chronic respiratory disease (0·6 years [7%] for men and 1·2 years [15%] for women).
Our findings suggest that increasing the adoption of these five healthy lifestyle factors through public health interventions could be associated with substantial gains in life expectancy in the Chinese population.
National Natural Science Foundation of China, National Key Research and Development Program of China, Kadoorie Charitable Foundation, UK Wellcome Trust.
提高预期寿命是“健康中国 2030 规划”的目标之一。本研究旨在调查中国成年人的生活方式与预期寿命之间的关联程度。
我们使用前瞻性中国慢性病前瞻性研究(CKB)来评估与单个和综合生活方式因素相关的死亡率(从不吸烟或因非疾病原因戒烟、不过度饮酒、积极运动、健康饮食习惯和健康体型)。排除患有冠心病、中风、癌症或 BMI 数据缺失的参与者。对于慢性呼吸道疾病的分析,排除患有慢性阻塞性肺疾病或哮喘的参与者。我们使用来自中国营养与健康监测(CNHS;2015 年)的数据来估计生活方式因素的全国流行率,并从全球疾病、伤害和风险因素研究(2015 年)中得出死亡率。我们结合了这三个数据源,使用生命表法根据不同水平的生活方式因素来估计 30 岁个体的预期寿命。使用 Arriaga 方法分析了预期寿命差异的原因分解。
在排除 CKB 中基线时患有冠心病、中风、癌症或 BMI 数据缺失的参与者后,共纳入 487209 名参与者进行主要分析。对于慢性呼吸道疾病相关分析,还排除了基线时患有 COPD 或哮喘的参与者,共纳入 451233 名有数据可供分析的参与者。使用来自 2015 年 CNHS 的 171127 名 30-84 岁成年人的数据来估计与生活方式相关因素的性别特异性和年龄特异性流行率。在 CKB 中位随访 11.1 年(IQR 10.2-12.1)期间,记录了 42496 例死亡。与 0-1 个低风险因素的参与者相比,采用五个低风险因素的参与者的全因死亡率调整后的危险比(aHR)为 0.38(95%CI 0.34-0.43),心血管疾病死亡率 aHR 为 0.37(0.30-0.46),癌症死亡率 aHR 为 0.47(0.39-0.56),慢性呼吸道疾病死亡率 aHR 为 0.30(0.14-0.64)。0-1 个低风险因素的个体在 30 岁时的预期寿命平均为男性 41.7 岁(95%CI 41.5-42.0),女性 47.3 岁(46.6-48.0)。对于所有五个低风险因素的个体,30 岁时的预期寿命为男性 50.5 岁(95%CI 48.5-52.4),女性 55.4 岁(53.5-57.4);意味着男性的差异为 8.8 岁(95%CI 6.8-10.7),女性的差异为 8.1 岁(6.5-9.9)。男性和女性的估计延长寿命主要归因于心血管疾病死亡率的降低(男性 2.4 年[总延长寿命的 27%],女性 3.7 年[46%]),癌症死亡率的降低(男性 2.6 年[30%],女性 0.9 年[11%]),和慢性呼吸道疾病死亡率的降低(男性 0.6 年[7%],女性 1.2 年[15%])。
我们的研究结果表明,通过公共卫生干预措施增加对这五种健康生活方式因素的采用,可能会使中国人口的预期寿命得到显著提高。
国家自然科学基金,国家重点研发计划,中国宋庆龄基金会,英国惠康基金会。