Section Medical Psychology and Psychotherapy, Department of Psychiatry, Erasmus MC, PO Box 2040, 3000 CA, Rotterdam, The Netherlands.
EuroQol Group, Rotterdam, The Netherlands.
Pharmacoeconomics. 2022 Nov;40(11):1081-1093. doi: 10.1007/s40273-022-01172-4. Epub 2022 Aug 5.
The aim of this study was to compare the responsiveness of EQ-5D-3L (3L) with EQ-5D-5L (5L) descriptive systems and value sets in two independent samples (rehabilitation and stroke patients).
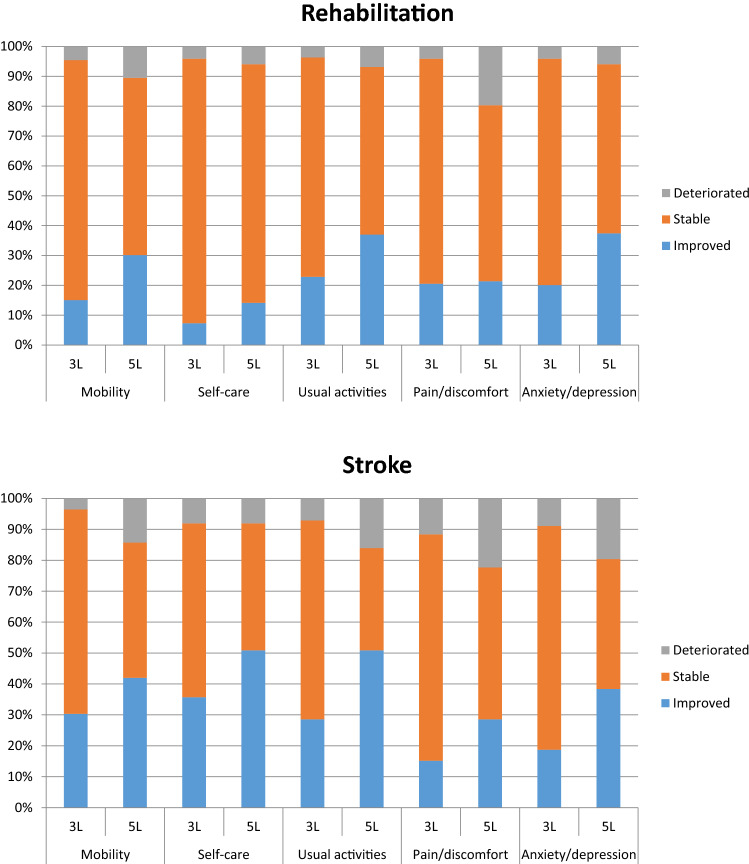
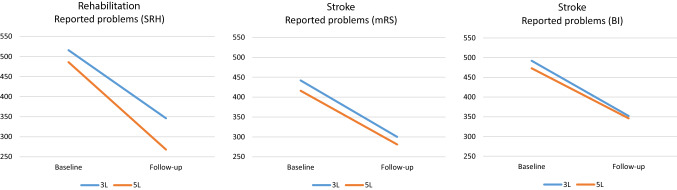
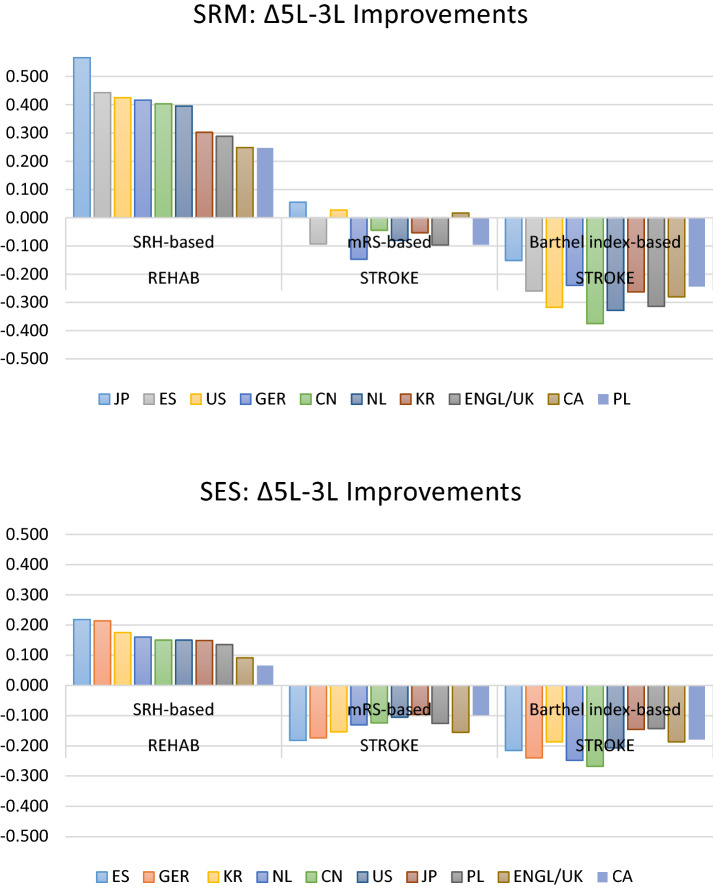
Descriptive system results were compared cross-sectionally, and descriptive responsiveness was tested by calculating changed level responses ('moves') from baseline to follow-up, proportion of improved patients, Paretian Classification of Health Change (PCHC), and probability of superiority (PS). Responsiveness of values based on nine country-specific value sets was assessed by standardized response mean (SRM) and standardized effect size (SES). Relative efficiency of 5L over 3L was assessed by calculating ratios of the SRM and SES statistics.
Descriptive comparisons confirmed earlier evidence and showed a consistent overestimation of health problems in 3L. Descriptive responsiveness improved with 5L in terms of moves per respondent, proportions of improved patients and PS, whereas PCHC showed mixed results. Better value responsiveness statistics were observed for 5L in rehabilitation patients for all value sets. In stroke patients, 3L showed better responsiveness statistics compared with 5L. Relative efficiency results were moderately to strongly better with 5L for rehabilitation, and slightly to moderately better with 3L for stroke.
Descriptive results were the main driver of 3L-5L responsiveness differences. Responsiveness of 3L was influenced by the 'confined to bed' label and the overestimation bias of 3L, which affected all responsiveness results. This may impact quality-adjusted life-year (QALY) estimations, leading to over- or underestimations of QALYs gained, depending on the condition and condition severity. QALY calculations based on 5L data will result in more accurate estimates.
本研究旨在比较 EQ-5D-3L(3L)和 EQ-5D-5L(5L)描述性系统在两个独立样本(康复和中风患者)中的反应能力。
横向比较描述性系统的结果,并通过计算从基线到随访的变化水平反应(“移动”)、改善患者的比例、健康变化帕累托分类(PCHC)和优势概率(PS)来测试描述性反应能力。基于九个国家特定价值集的价值反应能力通过标准化反应均值(SRM)和标准化效应大小(SES)进行评估。通过计算 SRM 和 SES 统计量的比值来评估 5L 相对于 3L 的相对效率。
描述性比较证实了早期的证据,并表明 3L 对健康问题的估计存在一致的高估。5L 在移动人数、改善患者比例和 PS 方面提高了描述性反应能力,而 PCHC 则显示出混合结果。对于康复患者,所有价值集都观察到 5L 的更好的价值反应能力统计数据。对于中风患者,与 5L 相比,3L 显示出更好的反应能力统计数据。对于康复患者,5L 的相对效率结果在中度到高度上更好,对于中风患者,3L 的相对效率结果在轻度到中度上更好。
描述性结果是 3L-5L 反应能力差异的主要驱动因素。3L 的反应能力受到“卧床”标签和 3L 的高估偏差的影响,这影响了所有反应能力结果。这可能会影响质量调整生命年(QALY)的估计,导致 QALY 增益的高估或低估,具体取决于病情和病情严重程度。基于 5L 数据的 QALY 计算将产生更准确的估计。