Karolinska Institutet, Department of Clinical Science Intervention and Technology, Division of Ear, Nose and Throat Diseases, Karolinska University Hospital, Huddinge, 141 86, Stockholm, Sweden.
Department of Otorhinolaryngology and Head and Neck Surgery and Department of Ophthalmology, Erasmus University Medical Center, Rotterdam, The Netherlands.
BMC Pediatr. 2022 Aug 5;22(1):473. doi: 10.1186/s12887-022-03218-0.
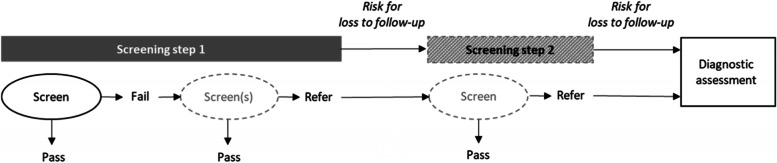
An effective newborn hearing screening programme has low referral rate and low loss to follow-up (LTFU) rate after referral from initial screening. This systematic review identified studies evaluating the effect of protocol and programme factors on these two outcomes, including the screening method used and the infant group.
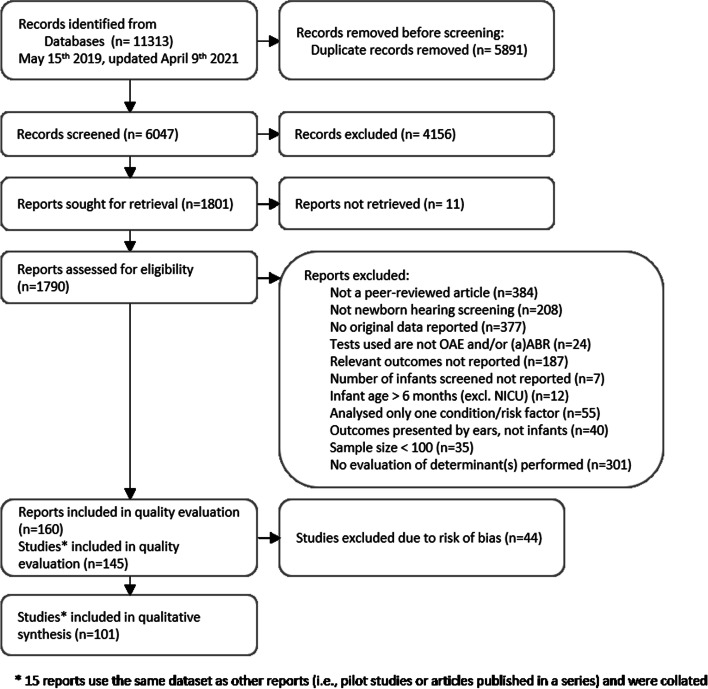
Five databases were searched (latest: April 2021). Included studies reported original data from newborn hearing screening and described the target outcomes against a protocol or programme level factor. Studies were excluded if results were only available for one risk condition, for each ear, or for < 100 infants, or if methodological bias was observed. Included studies were evaluated for quality across three domains: sample, screening and outcome, using modified criteria from the Ottawa-Newcastle and QUADAS-2 scales. Findings from the included studies were synthesised in tables, figures and text.
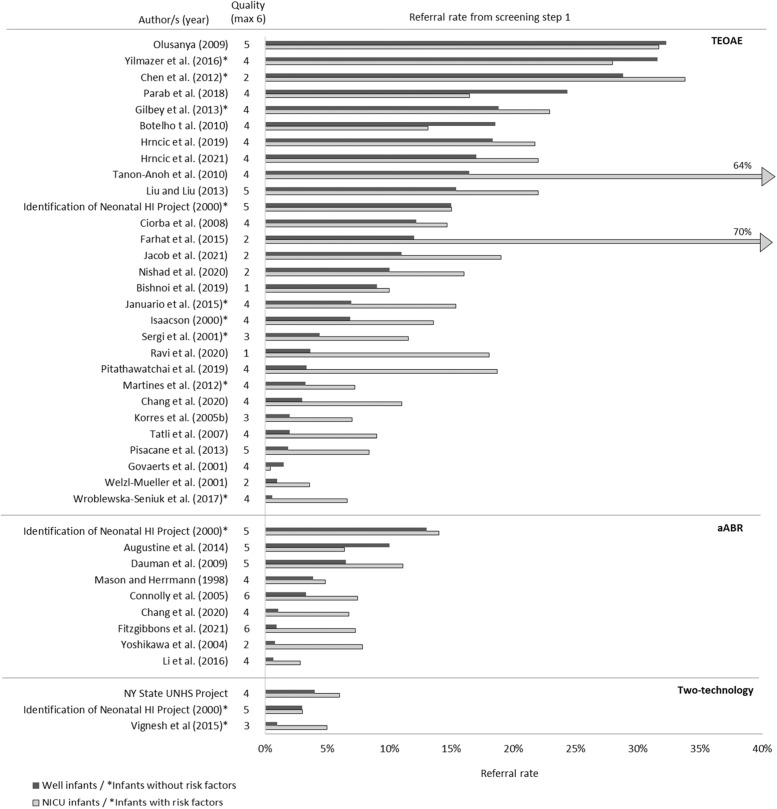
Fifty-eight studies reported on referral rate, 8 on LTFU rate, and 35 on both. Only 15 studies defined LTFU. Substantial diversity in referral and LTFU rate was observed across studies. Twelve of fourteen studies that evaluated screening method showed lower referral rates with aABR compared to TEOAE for well babies (WB). Rescreening before hospital discharge and screening after 3 days of age reduced referral rates. Studies investigating LTFU reported lower rates for programmes that had audiologist involvement, did not require fees for step 2, were embedded in a larger regional or national programme, and scheduled follow-up in a location accessible to the families. In programmes with low overall LTFU, higher LTFU was observed for infants from the NICU compared to WB.
Although poor reporting and exclusion of non-English articles may limit the generalisability from this review, key influential factors for referral and LTFU rates were identified. Including aABR in WB screening can effectively reduce referral rates, but it is not the only solution. The reported referral and LTFU rates vary largely across studies, implying the contribution of several parameters identified in this review and the context in which the programme is performed. Extra attention should be paid to infants with higher risk for hearing impairment to ensure their return to follow-up.
有效的新生儿听力筛查计划具有较低的转诊率和较低的随访损失率(LTFU),尤其是在初始筛查后。本系统评价确定了评估方案和计划因素对这两个结果的影响的研究,包括所使用的筛查方法和婴儿组。
在五个数据库中进行了搜索(最新日期:2021 年 4 月)。纳入的研究报告了新生儿听力筛查的原始数据,并针对方案或计划水平因素描述了目标结果。如果仅针对一种风险情况、每只耳朵或 <100 名婴儿提供结果,或者如果观察到方法学偏倚,则排除研究。使用来自渥太华-纽卡斯尔和 QUADAS-2 量表的修改标准,对纳入研究的三个领域(样本、筛查和结果)进行了质量评估。使用表格、图表和文本综合了纳入研究的结果。
58 项研究报告了转诊率,8 项研究报告了 LTFU 率,35 项研究报告了两者的情况。只有 15 项研究定义了 LTFU。研究之间的转诊率和 LTFU 率差异很大。14 项评估筛查方法的研究中有 12 项研究表明,对于健康婴儿(WB),aABR 与 TEOAE 相比,转诊率较低。在出院前进行重新筛查和在出生后 3 天进行筛查可降低转诊率。研究 LTFU 的报告显示,有听力学家参与、第二阶段不收取费用、嵌入更大的区域或国家计划、以及在家庭可及的地点安排随访的计划,其 LTFU 率较低。在总体 LTFU 较低的计划中,与 WB 婴儿相比,NICU 婴儿的 LTFU 率更高。
尽管报告不佳和排除非英语文章可能会限制本综述的普遍性,但确定了转诊率和 LTFU 率的关键影响因素。在 WB 筛查中包括 aABR 可以有效地降低转诊率,但这不是唯一的解决方案。研究之间的转诊率和 LTFU 率差异很大,这意味着本综述中确定的几个参数以及计划实施的背景都有贡献。应特别注意听力障碍风险较高的婴儿,以确保他们能回来随访。