University of Exeter College of Medicine and Health, Exeter, UK.
NIHR ARC South West Peninsula (PenARC), College of Medicine and Health, University of Exeter, Exeter, England.
BMC Med Res Methodol. 2022 Aug 6;22(1):216. doi: 10.1186/s12874-022-01691-w.
The Randomised Evaluation of COVID-19 Therapy (RECOVERY) trial is aimed at addressing the urgent need to find effective treatments for patients hospitalised with suspected or confirmed COVID-19. The trial has had many successes, including discovering that dexamethasone is effective at reducing COVID-19 mortality, the first treatment to reach this milestone in a randomised controlled trial. Despite this, it continues to use standard or 'fixed' randomisation to allocate patients to treatments. We assessed the impact of implementing response adaptive randomisation within RECOVERY using an array of performance measures, to learn if it could be beneficial going forward. This design feature has recently been implemented within the REMAP-CAP platform trial.
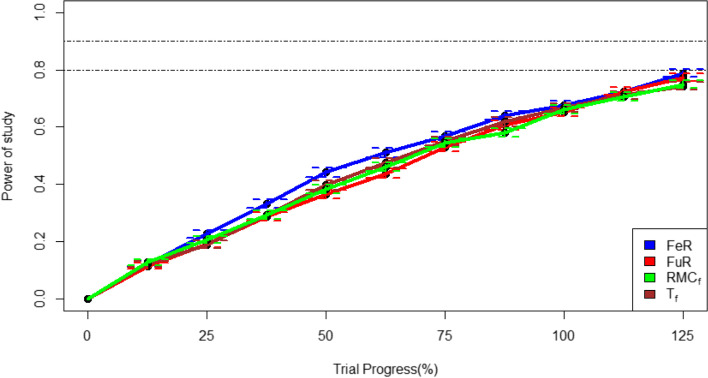
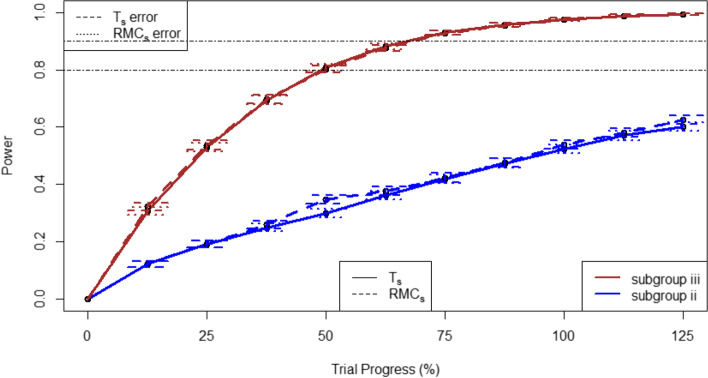
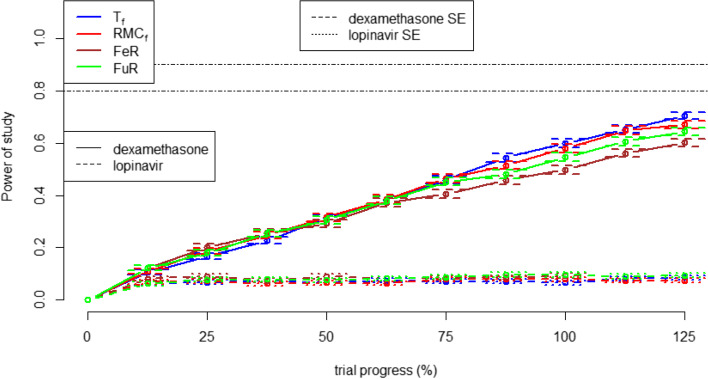
Trial data was simulated to closely match the data for patients allocated to standard care, dexamethasone, hydroxychloroquine, or lopinavir-ritonavir in the RECOVERY trial from March-June 2020, representing four out of five arms tested throughout this period. Trials were simulated in both a two-arm trial setting using standard care and dexamethasone, and a four-arm trial setting utilising all above treatments. Two forms of fixed randomisation and two forms of response-adaptive randomisation were tested. In the two-arm setting, response-adaptive randomisation was implemented across both trial arms, whereas in the four-arm setting it was implemented in the three non-standard care arms only. In the two-arm trial, randomisation strategies were performed at the whole trial level as well as within three pre-specified patient subgroups defined by patients' respiratory support level.
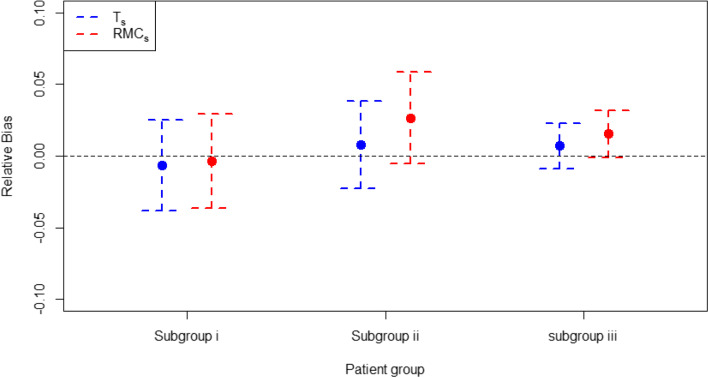
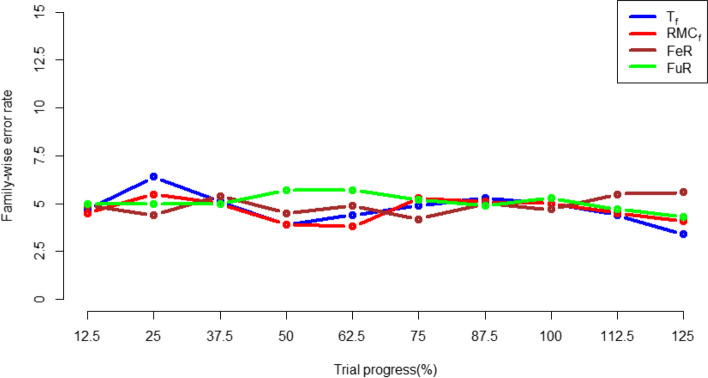
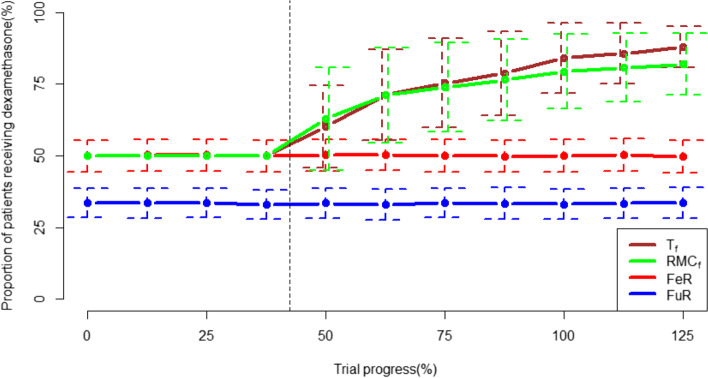
All response-adaptive randomisation strategies led to more patients being given dexamethasone and a lower mortality rate in the trial. Subgroup specific response-adaptive randomisation reduced mortality rates even further. In the two-arm trial, response-adaptive randomisation reduced statistical power compared to FR, with subgroup level adaptive randomisation exhibiting the largest power reduction. In the four-arm trial, response-adaptive randomisation increased statistical power in the dexamethasone arm but reduced statistical power in the lopinavir arm. Response-adaptive randomisation did not induce any meaningful bias in treatment effect estimates nor did it cause any inflation in the type 1 error rate.
Using response-adaptive randomisation within RECOVERY could have increased the number of patients receiving the optimal COVID-19 treatment during the trial, while reducing the number of patients needed to attain the same study power as the original study. This would likely have reduced patient deaths during the trial and lead to dexamethasone being declared effective sooner. Deciding how to balance the needs of patients within a trial and future patients who have yet to fall ill is an important ethical question for the trials community to address. Response-adaptive randomisation deserves to be considered as a design feature in future trials of COVID-19 and other diseases.
随机评估 COVID-19 治疗试验(RECOVERY)旨在满足寻找有效治疗疑似或确诊 COVID-19 住院患者的迫切需求。该试验取得了许多成功,包括发现地塞米松可有效降低 COVID-19 死亡率,这是首个在随机对照试验中达到这一里程碑的治疗方法。尽管如此,它仍继续使用标准或“固定”随机化来分配患者接受治疗。我们使用一系列性能指标评估了在 RECOVERY 中实施适应性随机化的影响,以了解其是否具有前瞻性益处。这一设计特点最近已在 REMAP-CAP 平台试验中实施。
试验数据被模拟,以尽可能匹配 2020 年 3 月至 6 月期间 RECOVERY 试验中接受标准治疗、地塞米松、羟氯喹或洛匹那韦-利托那韦治疗的患者数据,这代表了在此期间测试的五个治疗臂中的四个。在标准治疗和地塞米松的二臂试验设置和使用所有上述治疗的四臂试验设置中模拟了试验。测试了两种固定随机化和两种适应性随机化形式。在二臂试验中,适应性随机化在两个试验臂中实施,而在四臂试验中仅在三个非标准治疗臂中实施。在二臂试验中,随机化策略在整个试验层面以及在三个预先指定的患者亚组中进行,这些亚组根据患者的呼吸支持水平定义。
所有适应性随机化策略都导致试验中接受地塞米松治疗的患者更多,死亡率更低。亚组特异性适应性随机化进一步降低了死亡率。在二臂试验中,与 FR 相比,适应性随机化降低了统计效力,亚组水平适应性随机化显示出最大的效力降低。在四臂试验中,适应性随机化增加了地塞米松臂的统计效力,但降低了洛匹那韦臂的统计效力。适应性随机化没有导致治疗效果估计的任何有意义的偏差,也没有导致 I 型错误率的膨胀。
在 RECOVERY 中使用适应性随机化可以在试验期间增加接受最佳 COVID-19 治疗的患者数量,同时减少达到与原始研究相同研究效力所需的患者数量。这可能会减少试验期间的患者死亡,并导致更早地宣布地塞米松有效。对于试验界来说,决定如何平衡试验中的患者需求和尚未患病的未来患者的需求是一个重要的伦理问题。适应性随机化值得作为 COVID-19 和其他疾病未来试验的设计特点加以考虑。