Department of Intensive Care Medicine, Radboud University Medical Center, Postbus 9101, 6500 HB, Nijmegen, The Netherlands.
Department of Intensive Care Medicine, Amsterdam UMC Location University of Amsterdam, Amsterdam, Netherlands.
Crit Care. 2022 Aug 9;26(1):244. doi: 10.1186/s13054-022-04118-6.
A greater understanding of disease heterogeneity may facilitate precision medicine for coronavirus disease 2019 (COVID-19). Previous work identified four distinct clinical phenotypes associated with outcome and treatment responses in non-COVID-19 sepsis patients, but it is unknown if and how these phenotypes are recapitulated in COVID-19 sepsis patients.
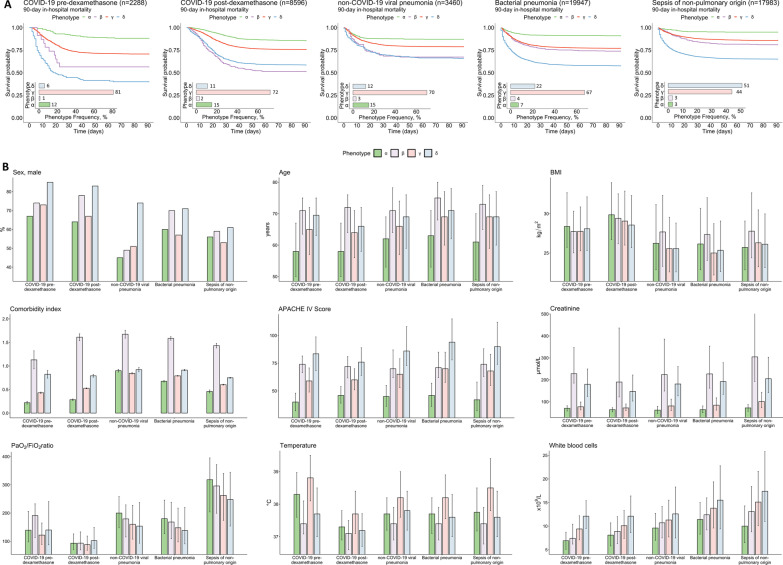
We applied the four non-COVID-19 sepsis phenotypes to a total of 52,274 critically ill patients, comprising two cohorts of COVID-19 sepsis patients (admitted before and after the introduction of dexamethasone as standard treatment) and three non-COVID-19 sepsis cohorts (non-COVID-19 viral pneumonia sepsis, bacterial pneumonia sepsis, and bacterial sepsis of non-pulmonary origin). Differences in proportions of phenotypes and their associated mortality were determined across these cohorts.
Phenotype distribution was highly similar between COVID-19 and non-COVID-19 viral pneumonia sepsis cohorts, whereas the proportion of patients with the δ-phenotype was greater in both bacterial sepsis cohorts compared to the viral sepsis cohorts. The introduction of dexamethasone treatment was associated with an increased proportion of patients with the δ-phenotype (6% vs. 11% in the pre- and post-dexamethasone COVID-19 cohorts, respectively, p < 0.001). Across the cohorts, the α-phenotype was associated with the most favorable outcome, while the δ-phenotype was associated with the highest mortality. Survival of the δ-phenotype was markedly higher following the introduction of dexamethasone (60% vs 41%, p < 0.001), whereas no relevant differences in survival were observed for the other phenotypes among COVID-19 patients.
Classification of critically ill COVID-19 patients into clinical phenotypes may aid prognostication, prediction of treatment efficacy, and facilitation of personalized medicine.
对疾病异质性的更深入了解可能有助于为 2019 年冠状病毒病(COVID-19)提供精准医疗。之前的研究在非 COVID-19 败血症患者中确定了与结局和治疗反应相关的四个不同临床表型,但尚不清楚这些表型是否以及如何在 COVID-19 败血症患者中再现。
我们将这四个非 COVID-19 败血症表型应用于总共 52274 名危重症患者,其中包括 COVID-19 败血症患者的两个队列(在使用地塞米松作为标准治疗之前和之后入院)和三个非 COVID-19 败血症队列(非 COVID-19 病毒性肺炎败血症、细菌性肺炎败血症和非肺部来源的细菌性败血症)。我们确定了这些队列中表型的比例及其相关死亡率的差异。
COVID-19 与非 COVID-19 病毒性肺炎败血症队列之间的表型分布非常相似,而在两个细菌性败血症队列中,δ-表型患者的比例均高于病毒性败血症队列。地塞米松治疗的引入与 δ-表型患者的比例增加有关(COVID-19 前和地塞米松治疗后队列分别为 6%和 11%,p<0.001)。在所有队列中,α-表型与最佳结局相关,而 δ-表型与最高死亡率相关。地塞米松引入后,δ-表型的生存率明显更高(60%对 41%,p<0.001),而 COVID-19 患者中其他表型的生存率没有观察到相关差异。
对危重症 COVID-19 患者进行临床表型分类可能有助于预后判断、治疗效果预测和促进个体化医疗。