Ceriani Elisa, Pitino Annalisa, Radovanovic Dejan, Salvi Emanuele, Matone Maddalena, Teatini Thomas, Gidaro Antonio, Tripepi Giovanni, Santus Pierachille, Gori Mercedes, Cogliati Chiara
Department of Internal Medicine, L. Sacco Hospital, Università Degli Studi di Milano, Via GB Grassi, 20157 Milano, Italy.
Institute of Clinical Physiology (IFC-CNR), Section of Rome, 00185 Rome, Italy.
J Clin Med. 2022 Jul 30;11(15):4454. doi: 10.3390/jcm11154454.
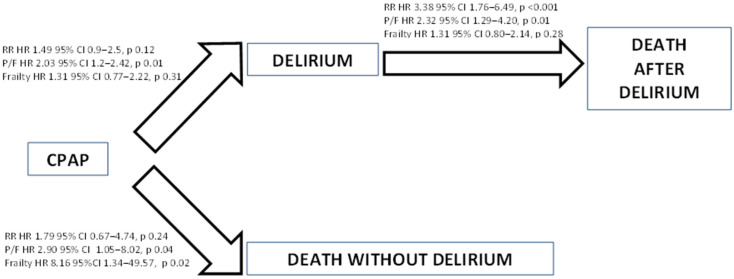
The elderly population represents a high percentage of patients hospitalized for COVID-19 pneumonia and severe respiratory failure, for whom CPAP may be a treatment option. The aim of this study was to describe the CPAP support modalities and to explore factors associated with CPAP failure. In this retrospective study, 110 consecutive patients aged ≥ 75 years were enrolled. Median frailty score, baseline partial arterial pressure of oxygen to fraction of inspired oxygen ratio (P/F), and respiratory rate (RR) were 5, 108, and 30 cycles/min, respectively. Of the 110 patients that began CPAP treatment, 17 patients died within 72 h from baseline, while in 2 patients, CPAP was withdrawn for clinical improvement. Thus, of the 91 patients still on CPAP at day 3, 67% of them needed continuous CPAP delivery. Patients with RR ≥ 30 and with frailty score ≥ 5 had an odds ratio of continuous CPAP needing of 3 and 4, respectively. Patients unable to tolerate CPAP-free periods demonstrated higher mortality risk as compared to those able to tolerate intermittent CPAP (OR: 6.04, 95% CI 2.38−16.46, p < 0.001). The overall in-hospital mortality was 63.6%. Delirium occurred in 59.1%, with a mortality rate in this subgroup of 83.1%. In a time-varying Cox model, the hazard ratio of death was 2.9 in patients with baseline RR ≥ 30 cycle/min, 2.4 in those with baseline P/F < 100. In the same model, the hazard ratio of death was 20 in patients with delirium and a frailty score < 5 and 8.8 in those without delirium and with frailty ≥ 5, indicating a competitive effect between these two variables on the death risk. Conclusions: Respiratory impairment, frailty, and delirium predict treatment failure, with the latter two factors demonstrating a competitive effect on mortality risk. CPAP support may represent a feasible therapeutic option in elderly patients, although chances of a therapeutic benefit are markedly reduced in case of severe respiratory impairment, very frail baseline condition or delirium occurrence.
老年人群在因新冠病毒肺炎和严重呼吸衰竭住院的患者中占比很高,对于他们而言,持续气道正压通气(CPAP)可能是一种治疗选择。本研究的目的是描述CPAP支持模式,并探索与CPAP失败相关的因素。在这项回顾性研究中,连续纳入了110名年龄≥75岁的患者。虚弱评分中位数、基线动脉血氧分压与吸入氧分数比值(P/F)以及呼吸频率(RR)分别为5、108和30次/分钟。在开始CPAP治疗的110名患者中,17名患者在基线后的72小时内死亡,而在2名患者中,因临床症状改善停用了CPAP。因此,在第3天仍在接受CPAP治疗的91名患者中,67%的患者需要持续进行CPAP通气。RR≥30且虚弱评分≥5的患者持续需要CPAP的比值比分别为3和4。与能够耐受间歇性CPAP的患者相比,无法耐受无CPAP时段的患者死亡风险更高(比值比:6.04,95%置信区间2.38−16.46,p<0.001)。总体住院死亡率为63.6%。谵妄发生率为59.1%,该亚组的死亡率为83.1%。在一个时变Cox模型中,基线RR≥30次/分钟的患者死亡风险比为2.9,基线P/F<100的患者为2.4。在同一模型中,发生谵妄且虚弱评分<5的患者死亡风险比为20,未发生谵妄且虚弱评分≥5的患者为8.8,这表明这两个变量对死亡风险存在竞争效应。结论:呼吸功能损害、虚弱和谵妄可预测治疗失败,后两个因素对死亡风险具有竞争效应。CPAP支持可能是老年患者的一种可行治疗选择,尽管在存在严重呼吸功能损害、基线身体状况非常虚弱或发生谵妄的情况下,治疗获益的机会会显著降低。