Department of Intensive Care Medicine, Maastricht University Medical Centre+, P. Debyelaan 25, P.O. Box 5800, 6202, AZ, Maastricht, The Netherlands.
Cardiovascular Research Institute Maastricht (CARIM), Maastricht University, Maastricht, The Netherlands.
BMC Anesthesiol. 2022 Aug 15;22(1):258. doi: 10.1186/s12871-022-01801-7.
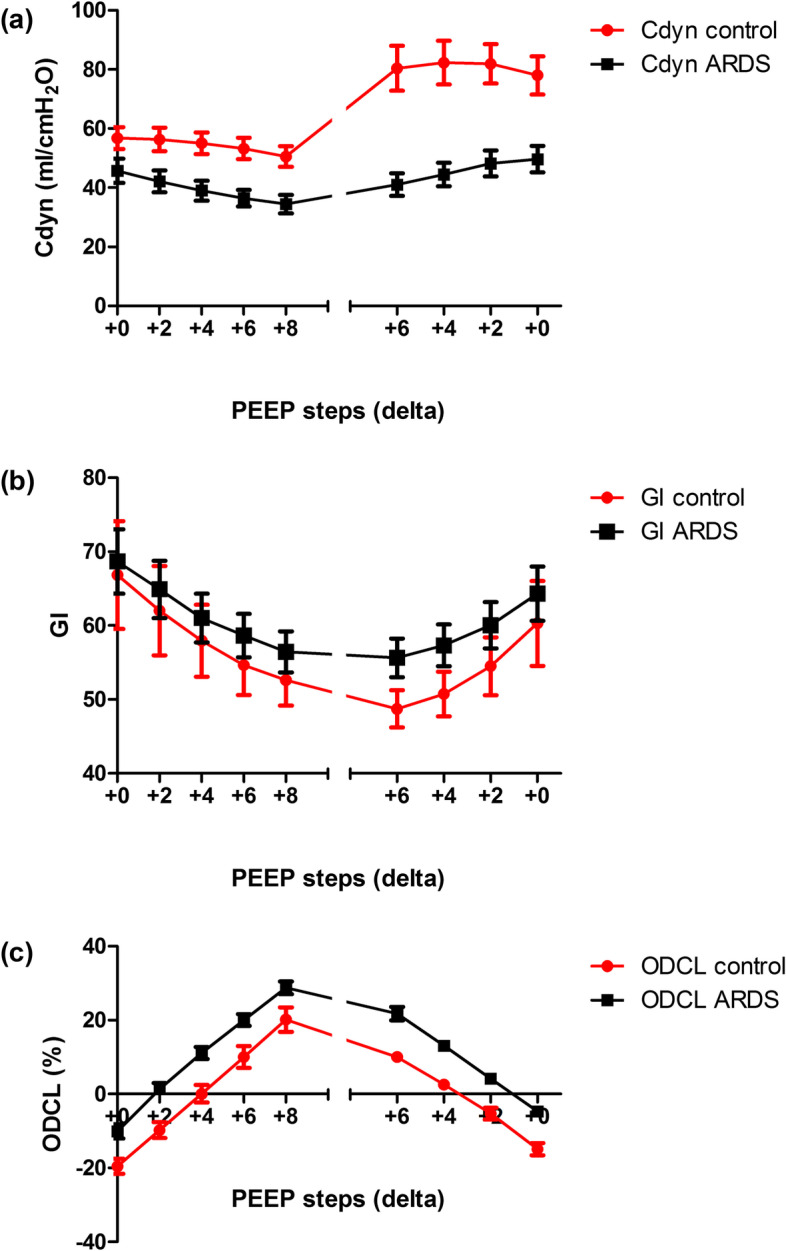
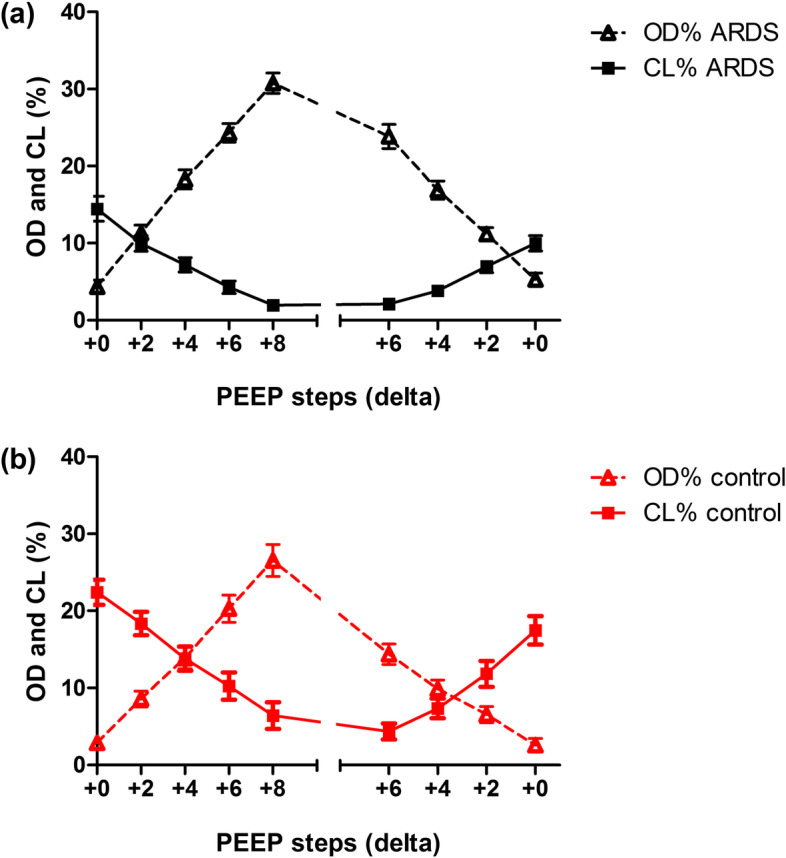
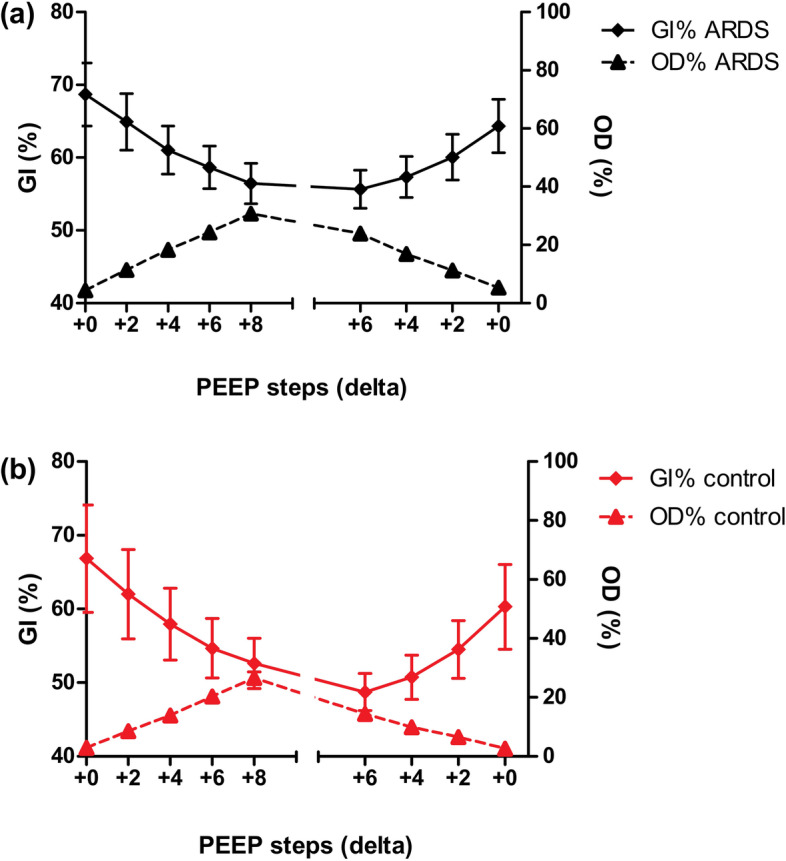
Electrical impedance tomography (EIT) visualises alveolar overdistension and alveolar collapse and enables optimisation of ventilator settings by using the best balance between alveolar overdistension and collapse (ODCL). Besides, the global inhomogeneity index (GI), measured by EIT, may also be of added value in determining PEEP. Optimal PEEP is often determined based on the best dynamic compliance without EIT at the bedside. This study aimed to assess the effect of a PEEP trial on ODCL, GI and dynamic compliance in patients with and without ARDS. Secondly, PEEP levels from "optimal PEEP" approaches by ODCL, GI and dynamic compliance are compared.
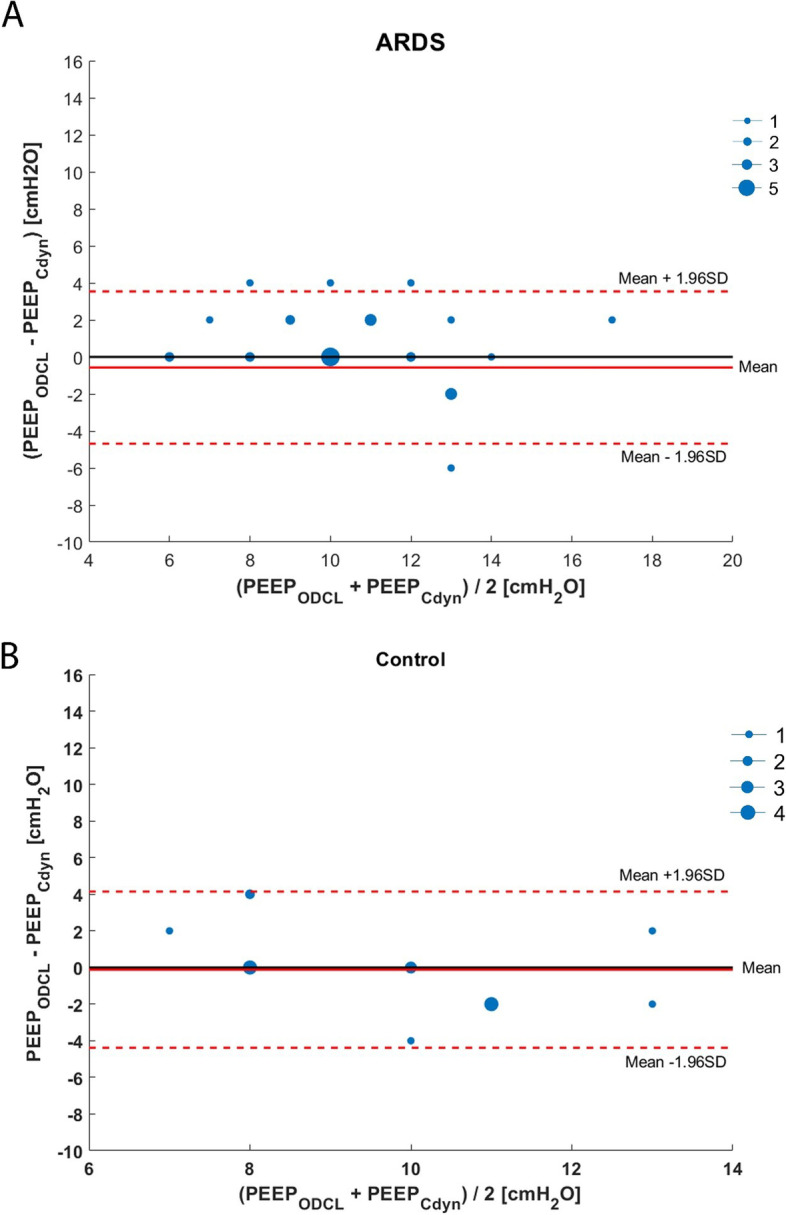
In 2015-2016, we included patients with ARDS using postoperative cardiothoracic surgery patients as a reference group. A PEEP trial was performed with four consecutive incremental followed by four decremental PEEP steps of 2 cmHO. Primary outcomes at each step were GI, ODCL and best dynamic compliance. In addition, the agreement between ODCL, GI, and dynamic compliance was determined for the individual patient.
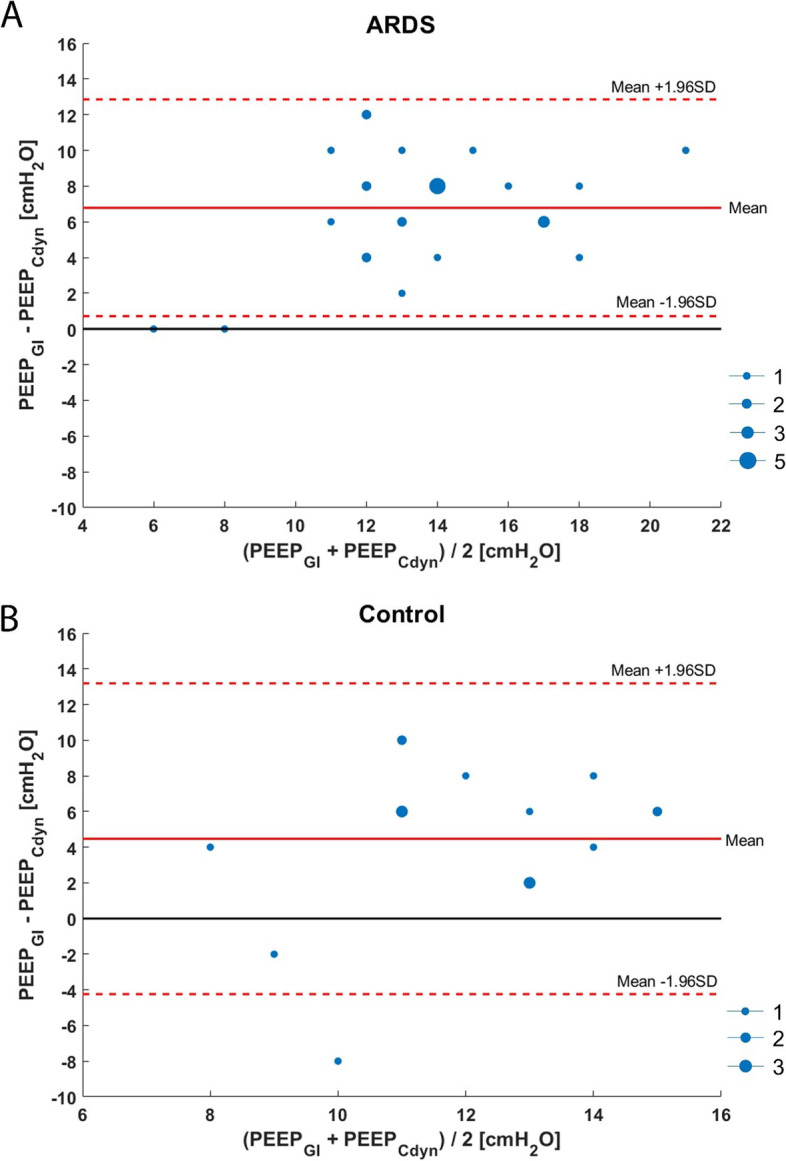
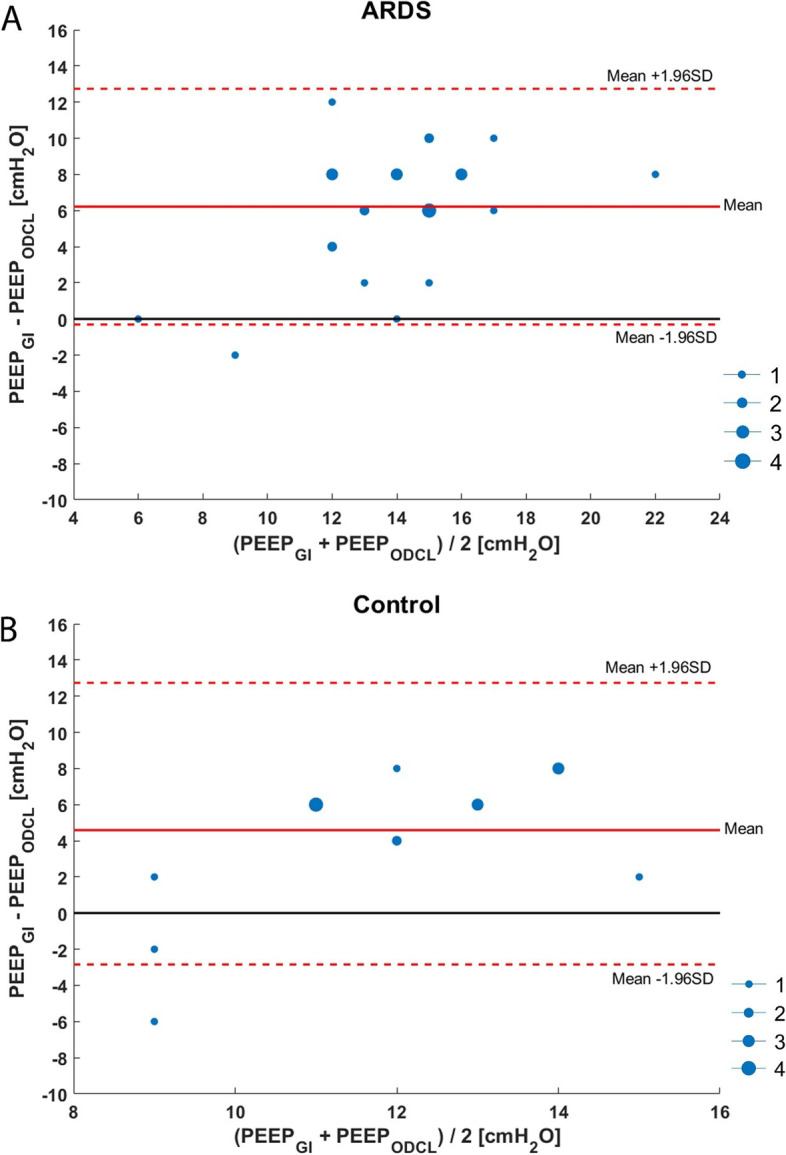
Twenty-eight ARDS and 17 postoperative cardiothoracic surgery patients were included. The mean optimal PEEP, according to best compliance, was 10.3 (±2.9) cmHO in ARDS compared to 9.8 (±2.5) cmHO in cardiothoracic surgery patients. Optimal PEEP according to ODCL was 10.9 (±2.5) in ARDS and 9.6 (±1.6) in cardiothoracic surgery patients. Optimal PEEP according to GI was 17.1 (±3.9) in ARDS compared to 14.2 (±3.4) in cardiothoracic surgery patients.
Currently, no golden standard to titrate PEEP is available. We showed that when using the GI, PEEP requirements are higher compared to ODCL and best dynamic compliance during a PEEP trial in patients with and without ARDS.
电阻抗断层成像(EIT)可可视化肺泡过度膨胀和肺泡萎陷,并通过使用肺泡过度膨胀和萎陷之间的最佳平衡来优化呼吸机设置(ODCL)。此外,EIT 测量的全局不均匀指数(GI)在确定 PEEP 方面也可能具有附加价值。最佳 PEEP 通常是基于床边无 EIT 时的最佳动态顺应性来确定的。本研究旨在评估在 ARDS 和非 ARDS 患者中进行 PEEP 试验对 ODCL、GI 和动态顺应性的影响。其次,比较基于 ODCL、GI 和动态顺应性的“最佳 PEEP”方法得出的 PEEP 水平。
在 2015-2016 年,我们纳入了使用术后心胸外科患者作为参考组的 ARDS 患者。进行了 PEEP 试验,有四个连续递增和四个递减 PEEP 步骤,每次增加或减少 2 cmHO。在每个步骤中,主要结局是 GI、ODCL 和最佳动态顺应性。此外,还确定了 ODCL、GI 和动态顺应性在个体患者中的一致性。
共纳入 28 例 ARDS 患者和 17 例术后心胸外科患者。根据最佳顺应性,ARDS 患者的最佳 PEEP 平均值为 10.3(±2.9)cmHO,而心胸外科患者为 9.8(±2.5)cmHO。根据 ODCL,ARDS 患者的最佳 PEEP 为 10.9(±2.5)cmHO,心胸外科患者为 9.6(±1.6)cmHO。根据 GI,ARDS 患者的最佳 PEEP 为 17.1(±3.9)cmHO,心胸外科患者为 14.2(±3.4)cmHO。
目前,尚无滴定 PEEP 的金标准。我们表明,在 ARDS 和非 ARDS 患者中进行 PEEP 试验时,与 ODCL 和最佳动态顺应性相比,使用 GI 时 PEEP 的需求更高。