Nuffield Department of Anaesthesia, Oxford University Hospitals NHS Trust, Oxford, UK.
Department of Anaesthesia, Royal Berkshire Hospital, Reading, UK.
Anaesthesia. 2022 Nov;77(11):1251-1258. doi: 10.1111/anae.15840. Epub 2022 Aug 16.
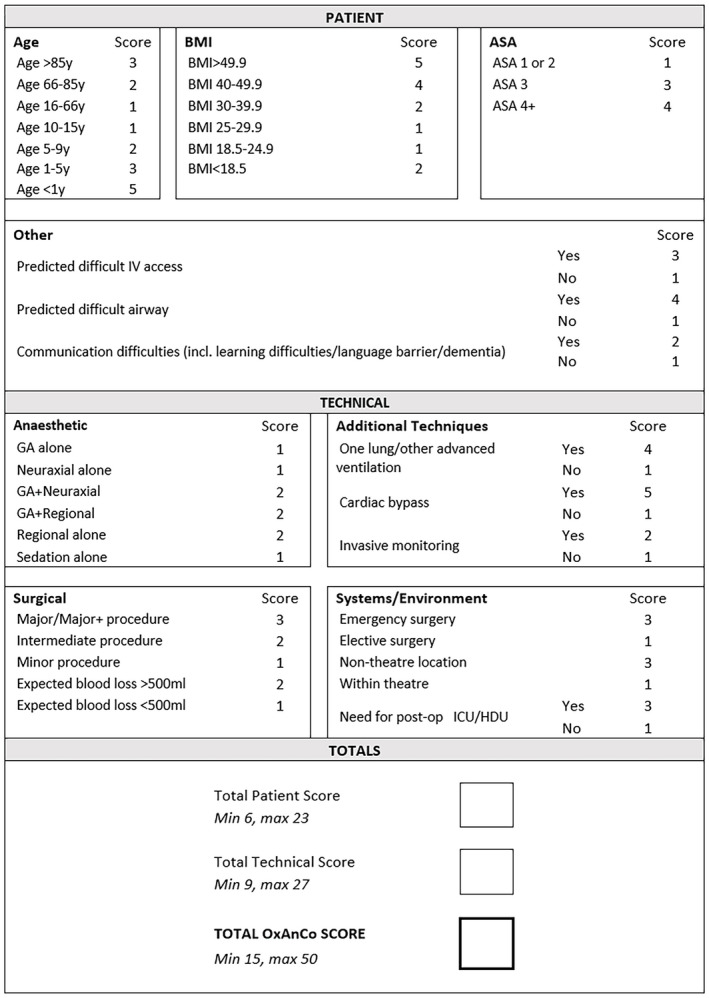
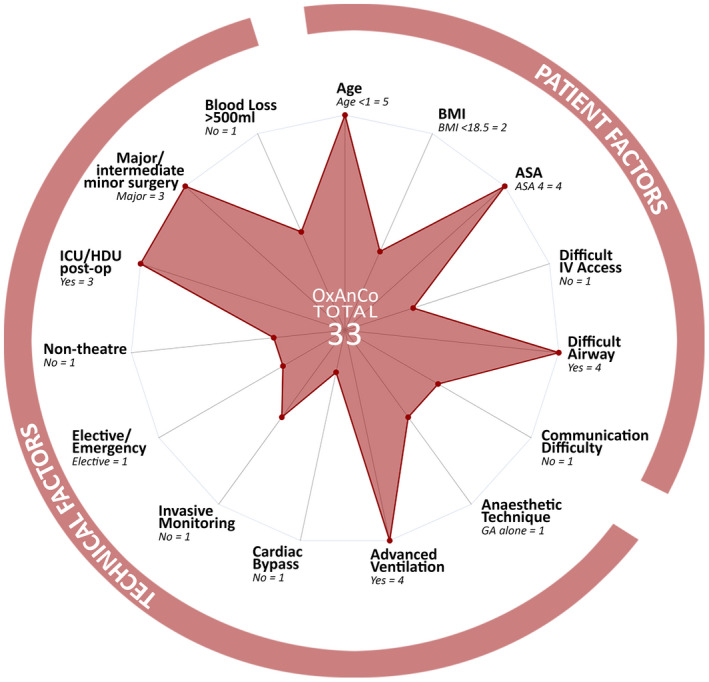
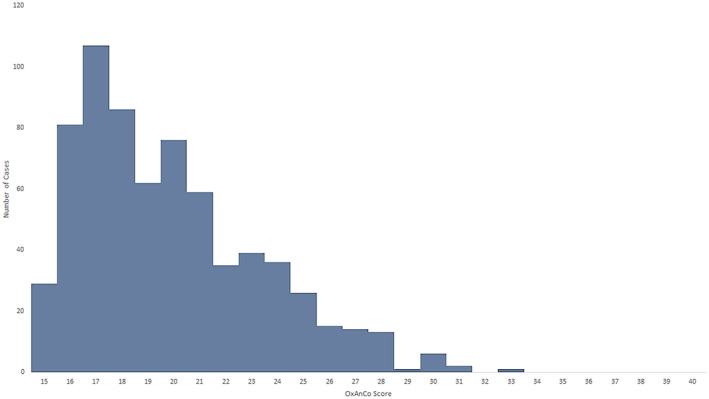
Increasing demand for surgery and anaesthesia has created an imperative to manage anaesthetic workforce and caseload. This may include changes to distribution of cases amongst anaesthetists of different grades, including non-physician anaesthetists. To achieve this safely, an assessment of case complexity is essential. We present a novel system for scoring complexity of cases in anaesthesia, the Oxford Anaesthetic Complexity score. This integrates patient, anaesthetic, surgical and systems factors, and is different from assessments of risk. We adopted an end-user development approach to the design of the score, and validated it using a dataset of anaesthetic cases. Across 688 cases, the median (IQR [range]) complexity score was 19 (17-22 [15-33]). Cases requiring a consultant anaesthetist had a significantly higher median (IQR [range]) score than those requiring a senior trainee at 22 (20-25 [15-33]) vs. 19(17-21 [15-28]), p < 0.001. Cases undertaken in a tertiary acute hospital had a significantly higher score than those in a district general hospital, the median (IQR [range]) scores being 20 (17-22 [15-33]) vs. 17 (16-19 [17-28]), p < 0.001. Receiver-operating characteristic analysis showed good prediction of complexity sufficient to require a consultant anaesthetist, with area under the curve of 0.84. Any rise in complexity above baseline (score > 15) was strongly predictive of a case too complex for a junior trainee (positive predictive value 0.93). The Oxford Anaesthetic Complexity score can be used to match cases to different grades of anaesthetist, and can help in defining cases appropriate for the expanding non-physician anaesthetist workforce.
手术和麻醉需求的增加使得管理麻醉人员和病例量变得势在必行。这可能包括改变不同级别麻醉医师(包括非医师麻醉师)之间的病例分配。为了安全地实现这一目标,对病例复杂性进行评估至关重要。我们提出了一种新的麻醉病例复杂性评分系统,即牛津麻醉复杂性评分。该评分系统综合了患者、麻醉、手术和系统因素,与风险评估不同。我们采用终端用户开发方法来设计评分系统,并使用麻醉病例数据集对其进行验证。在 688 例病例中,中位数(IQR [范围])复杂性评分为 19(17-22 [15-33])。需要顾问麻醉师的病例中位数(IQR [范围])明显高于需要高级住院医师的病例,分别为 22(20-25 [15-33])与 19(17-21 [15-28]),p<0.001。在三级急症医院进行的病例比在地区综合医院进行的病例评分明显更高,中位数(IQR [范围])分别为 20(17-22 [15-33])与 17(16-19 [17-28]),p<0.001。受试者工作特征分析显示,该评分对需要顾问麻醉师的复杂性有较好的预测能力,曲线下面积为 0.84。任何高于基线的复杂性增加(评分>15)都强烈预示着该病例对初级住院医师来说过于复杂(阳性预测值 0.93)。牛津麻醉复杂性评分可用于将病例与不同级别的麻醉师匹配,并有助于定义适合非医师麻醉师队伍扩大的病例。