National Clinician Scholars Program, Yale School of Medicine, New Haven, Connecticut.
Department of Emergency Medicine, Yale School of Medicine, New Haven, Connecticut.
JAMA Health Forum. 2022 Jan 28;3(1):e214611. doi: 10.1001/jamahealthforum.2021.4611. eCollection 2022 Jan.
Low-income older adults who are dually eligible (DE) for Medicare and Medicaid often experience worse outcomes following hospitalization. Among other federal policies aimed at improving health for DE patients, Medicare has recently begun reporting disparities in within-hospital readmissions. The degree to which disparities for DE patients are owing to differences in community-level factors or, conversely, are amenable to hospital quality improvement, remains heavily debated.
To examine the extent to which within-hospital disparities in 30-day readmission rates for DE patients are ameliorated by state- and community-level factors.
In this retrospective cohort study, Centers for Medicare & Medicaid Services (CMS) Disparity Methods were used to calculate within-hospital disparities in 30-day risk-adjusted readmission rates for DE vs non-DE patients in US hospitals participating in Medicare. All analyses were performed in February and March 2019. The study included Medicare patients (aged ≥65 years) hospitalized for acute myocardial infarction (AMI), heart failure (HF), or pneumonia in 2014 to 2017.
Within-hospital disparities, as measured by the rate difference (RD) in 30-day readmission between DE vs non-DE patients following admission for AMI, HF, or pneumonia; variance across hospitals; and correlation of hospital RDs with and without adjustment for state Medicaid eligibility policies and community-level factors.
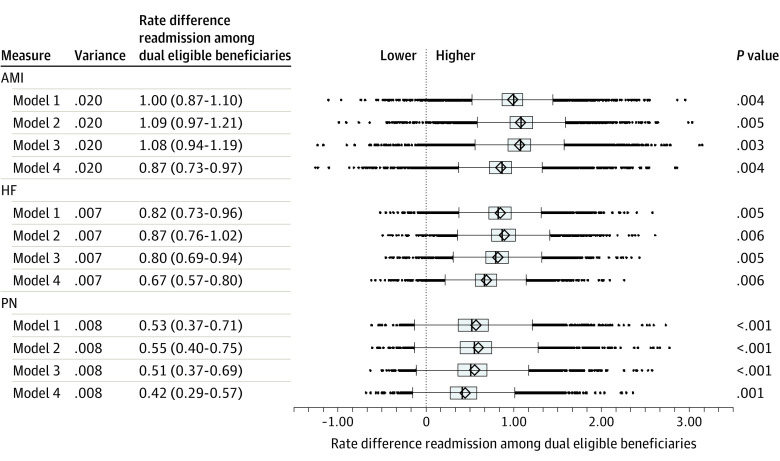
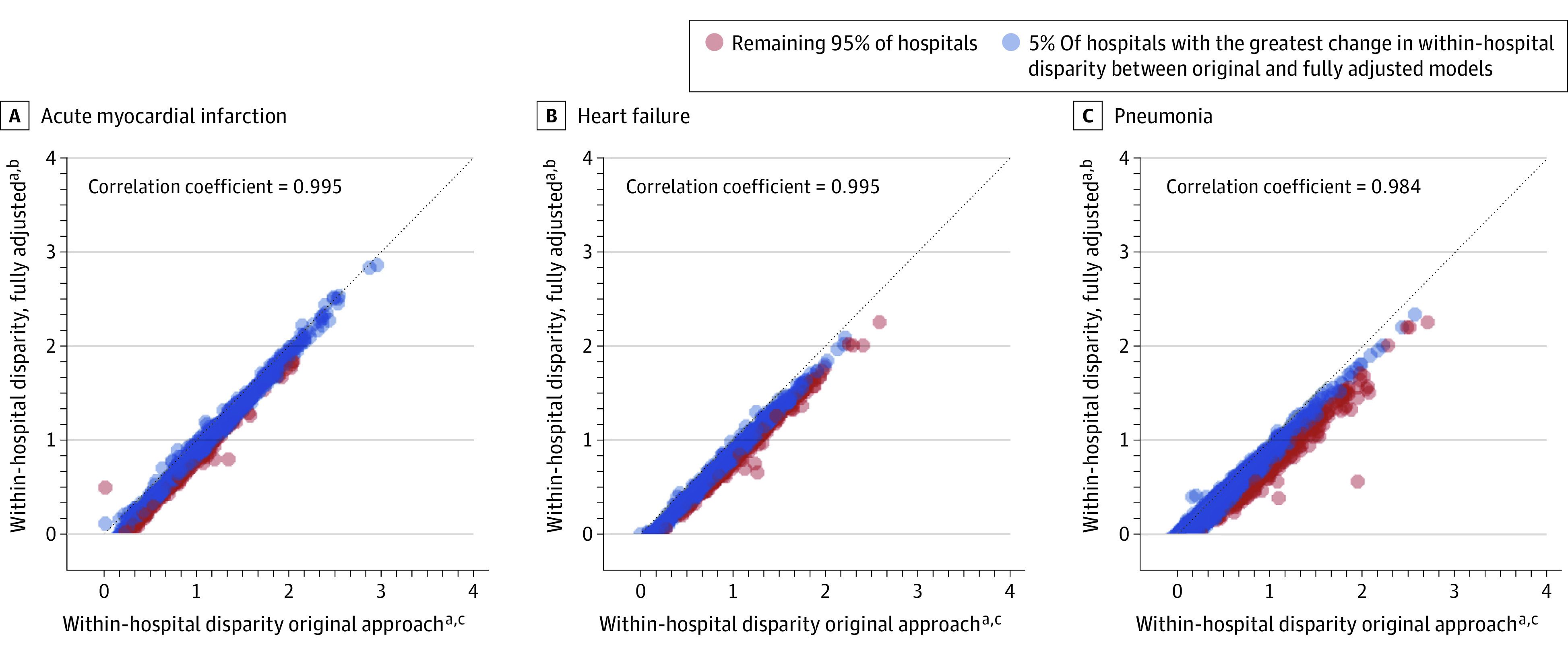
The final sample included 475 444 patients admitted for AMI, 898 395 for HF, and 1 214 282 for pneumonia, of whom 13.2%, 17.4%, and 23.0% were DE patients, respectively. Dually eligible patients had higher 30-day readmission rates relative to non-DE patients (RD >0) in 99.0% (AMI), 99.4% (HF), and 97.5% (pneumonia) of US hospitals. Across hospitals, the mean (IQR) RD between DE vs non-DE was 1.00% (0.87%-1.10%) for AMI, 0.82% (0.73%-0.96%) for HF, and 0.53% (0.37%-0.71%) for pneumonia. The mean (IQR) RD after adjustment for community-level factors was 0.87% (0.73%-0.97%) for AMI, 0.67% (0.57%-0.80%) for HF, and 0.42% (0.29%-0.57%) for pneumonia. Relative hospital rankings of corresponding within-hospital disparities before and after community-level adjustment were highly correlated (Pearson coefficient, 0.98).
In this cohort study, within-hospital disparities in 30-day readmission for DE patients were modestly associated with differences in state Medicaid policies and community-level factors. This suggests that remaining variation in these disparities should be the focus of hospital efforts to improve the quality of care transitions at discharge for DE patients in efforts to advance equity.
同时符合医疗保险和医疗补助资格的低收入老年患者在住院后往往会出现更差的预后。为改善双重资格患者的健康状况,联邦政府实施了其他多项政策,其中医疗保险最近开始报告医院内再入院的差异。双重资格患者的差异在多大程度上是由于社区层面因素造成的,或者相反,这些差异是否可以通过医院质量改进来解决,这仍然存在很大争议。
研究州和社区层面因素对双重资格患者 30 天内再入院率的院内差异的缓解程度。
设计、设置和参与者:本回顾性队列研究使用医疗保险和医疗补助服务中心(CMS)的差异方法,计算了美国医疗保险参与医院中,因急性心肌梗死(AMI)、心力衰竭(HF)或肺炎住院的双重资格与非双重资格患者的 30 天风险调整后再入院率的院内差异。所有分析均于 2019 年 2 月和 3 月进行。研究纳入了 2014 年至 2017 年因 AMI、HF 或肺炎住院的年龄≥65 岁的 Medicare 患者。
通过以下指标衡量院内差异:AMI、HF 和肺炎住院后,双重资格与非双重资格患者的 30 天再入院率差异(率差[RD]);医院间差异;以及医院 RD 与调整州医疗补助资格政策和社区层面因素前后的相关性。
最终纳入 475444 例因 AMI 入院、898395 例因 HF 入院和 1214282 例因肺炎入院的患者,其中分别有 13.2%、17.4%和 23.0%的患者为双重资格患者。在 99.0%(AMI)、99.4%(HF)和 97.5%(肺炎)的美国医院中,双重资格患者的 30 天再入院率高于非双重资格患者(RD>0)。在医院间,双重资格与非双重资格患者的平均(IQR)RD 分别为 1.00%(0.87%-1.10%)、0.82%(0.73%-0.96%)和 0.53%(0.37%-0.71%)。调整社区层面因素后,平均(IQR)RD 分别为 0.87%(0.73%-0.97%)、0.67%(0.57%-0.80%)和 0.42%(0.29%-0.57%)。在调整社区层面因素前后,相应的院内差异的医院相对排名高度相关(Pearson 系数,0.98)。
在本队列研究中,双重资格患者 30 天内再入院的院内差异与州医疗补助政策和社区层面因素的差异有一定关联。这表明,这些差异中剩余的差异应成为医院努力的重点,以改善出院时双重资格患者的护理过渡质量,从而推进公平性。