Office of Biostatistics and Epidemiology, Center for Biologics Evaluation and Research, Food and Drug Administration, Silver Spring, Maryland, United States of America.
Baylor Scott & White Research Institute, Dallas, TX, United States of America.
PLoS One. 2022 Aug 18;17(8):e0273223. doi: 10.1371/journal.pone.0273223. eCollection 2022.
Although frequently used in the early pandemic, data on the effectiveness of COVID-19 convalescent plasma (CCP) remain mixed. We investigated the effectiveness and safety of CCP in hospitalized COVID-19 patients in real-world practices during the first two waves of the pandemic in a multi-hospital healthcare system in Texas.
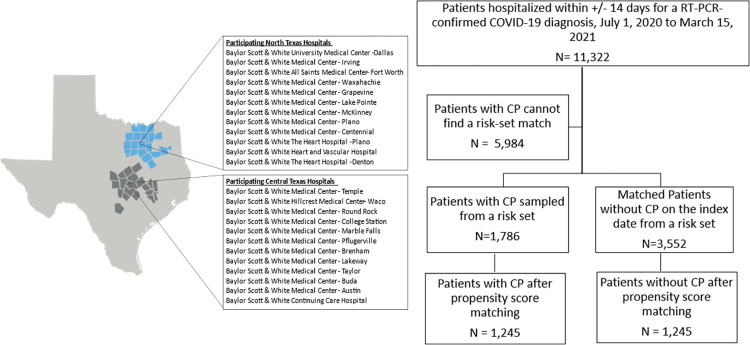
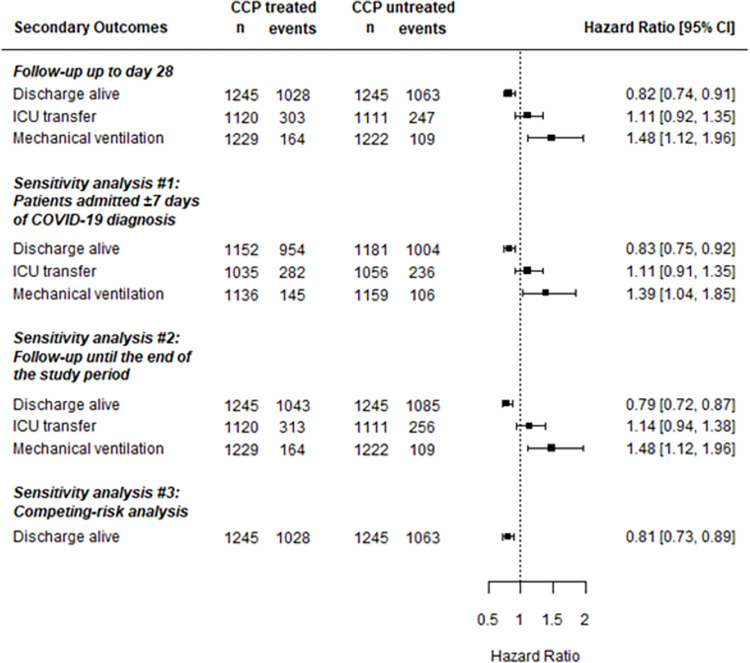
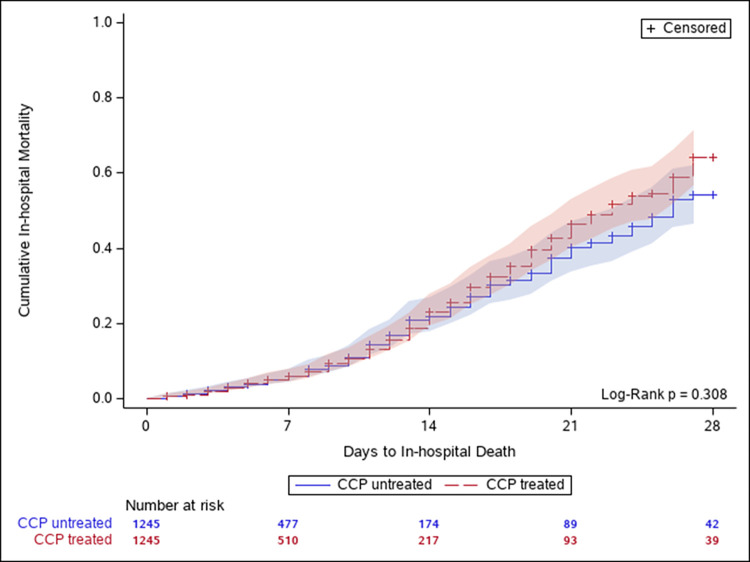
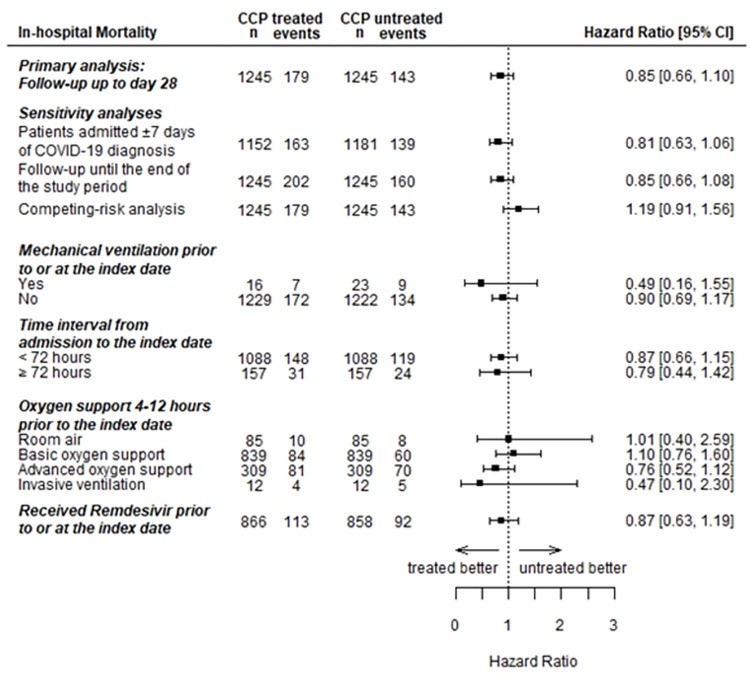
Among 11,322 hospitalized patients with confirmed COVID-19 infection from July 1, 2020 to April 15, 2021, we included patients who received CCP and matched them with those who did not receive CCP within ±2 days of the transfusion date across sites within strata of sex, age groups, days and use of dexamethasone from hospital admission to the match date, and oxygen requirements 4-12 hours prior to the match date. Cox proportional hazards model estimated hazard ratios (HRs) and 95% confidence intervals (CIs) for effectiveness outcomes in a propensity score 1:1 matched cohort. Pre-defined safety outcomes were described. We included 1,245 patients each in the CCP treated and untreated groups. Oxygen support was required by 93% of patients at the baseline. The pre-defined primary effectiveness outcome of 28-day in-hospital all-cause mortality (HR = 0.85; 95%CI: 0.66,1.10) were similar between treatment groups. Sensitivity and stratified analyses found similar null results. CCP-treated patients were less likely to be discharged alive (HR = 0.82; 95%CI: 0.74, 0.91), and more likely to receive mechanical ventilation (HR = 1.48; 95%CI: 1.12, 1.96). Safety outcomes were rare and similar between treatment groups.
The findings in this large, matched cohort of patients hospitalized with COVID-19 and mostly requiring oxygen support at the time of treatment, do not support a clinical benefit in 28-day in-hospital all-cause mortality for CCP. Future studies should assess the potential benefits with specifically high-titer units in perhaps certain subgroups of patients (e.g. those with early disease or immunocompromised).
虽然 COVID-19 恢复期血浆(CCP)在早期大流行期间经常被使用,但关于其疗效的数据仍然存在差异。我们在德克萨斯州的一个多医院医疗系统中,调查了在大流行的前两个波次中,CCP 在住院 COVID-19 患者中的疗效和安全性。
在 2020 年 7 月 1 日至 2021 年 4 月 15 日期间,我们纳入了 11322 名住院的 COVID-19 感染确诊患者,这些患者在接受 CCP 治疗的同时,还与在同一地点、同一性别、年龄组、从入院到匹配日期的地塞米松使用天数以及在匹配日期前 4-12 小时的氧气需求相匹配的患者进行了匹配。在倾向评分 1:1 匹配队列中,Cox 比例风险模型估计了疗效结局的风险比(HR)和 95%置信区间(CI)。描述了预先定义的安全性结局。在 CCP 治疗组和未治疗组中,我们分别纳入了 1245 名患者。基线时,93%的患者需要吸氧支持。28 天院内全因死亡率的预先定义的主要疗效结局(HR=0.85;95%CI:0.66,1.10)在治疗组之间相似。敏感性和分层分析发现了相似的无效结果。CP 治疗组的患者更有可能存活出院(HR=0.82;95%CI:0.74,0.91),更有可能接受机械通气(HR=1.48;95%CI:1.12,1.96)。安全性结局很少见,且在治疗组之间相似。
在这项针对住院 COVID-19 患者的大型匹配队列研究中,大多数患者在接受治疗时需要吸氧支持,结果并未支持 CCP 在 28 天院内全因死亡率方面的临床获益。未来的研究应该评估在特定高滴度单位的情况下,在某些特定亚组患者(例如早期疾病或免疫功能低下的患者)中,CP 可能带来的潜在获益。