Yu Haoting, Fu Jianhua, Feng Yong
Department of Pediatrics, Shengjing Hospital of China Medical University, Shenyang, China.
Front Pediatr. 2022 Aug 4;10:956952. doi: 10.3389/fped.2022.956952. eCollection 2022.
There remains controversy regarding vitamin D deficiency and bronchopulmonary dysplasia (BPD) in very low birth weight (VLBW) and extremely low birth weight (ELBW) preterm infants. This study aimed to determine the prevalence of vitamin D deficiency assessed by umbilical cord blood 25-hydroxyvitamin D [25(OH)D] in preterm infants in northeast China and to evaluate the ability and optimal threshold of 25(OH)D for predicting BPD.
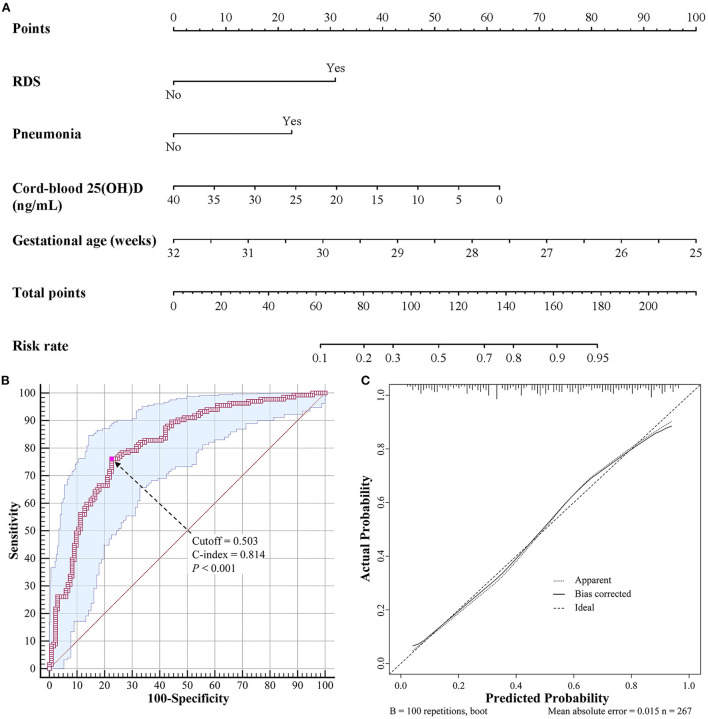
The clinical data of VLBW and ELBW preterm infants with known cord-blood 25(OH)D levels were analyzed retrospectively. Infants were divided into groups based on their cord-blood 25(OH)D levels and BPD diagnosis. Logistic regression was performed to assess the risk factors for BPD and a nomogram was established. Receiver operating characteristic (ROC) curve analysis was used to evaluate the optimal threshold of cord-blood 25(OH)D concentration for predicting BPD.
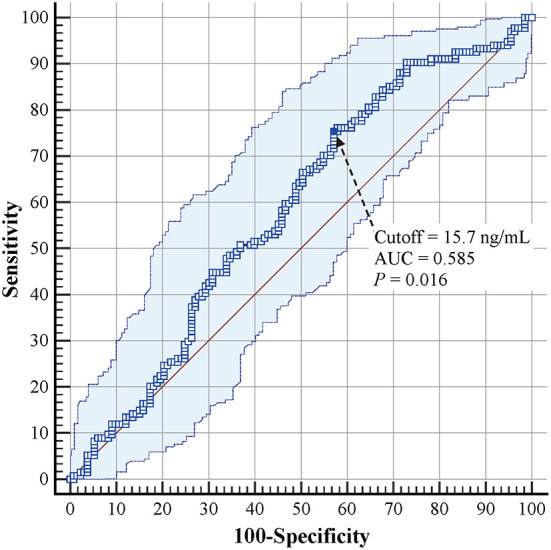
A total of 267 preterm infants were included, of which 225 (84.3%) exhibited vitamin D deficiency and 134 (50.2%) were diagnosed with BPD. The incidence of BPD was lower in the group with a 25(OH)D level of >20 ng/ml than in the other groups ( = 0.024). Infants with BPD had lower cord-blood 25(OH)D levels than those without BPD (11.6 vs. 13.6 ng/ml, = 0.016). The multivariate logistic regression model revealed that 25(OH)D levels (odds ratio [OR] = 0.933, 95% confidence interval [95% CI]: 0.891-0.977), gestational age (OR = 0.561, 95% CI: 0.425-0.740), respiratory distress syndrome (OR = 2.989, 95% CI: 1.455-6.142), and pneumonia (OR = 2.546, 95% CI: 1.398-4.639) were independent risk factors for BPD. A predictive nomogram containing these four risk factors was established, which had a C-index of 0.814. ROC curve analysis revealed that the optimal cutoff value of 25(OH)D for predicting BPD was 15.7 ng/ml (area under the curve = 0.585, 95% CI: 0.523-0.645, = 0.016), with a sensitivity of 75.4% and a specificity of 42.9%.
A cord-blood 25(OH)D level of <15.7 ng/ml was predictively valuable for the development of BPD. The nomogram established in this study can help pediatricians predict the risk of BPD more effectively and easily.
极低出生体重(VLBW)和超低出生体重(ELBW)早产儿的维生素D缺乏与支气管肺发育不良(BPD)之间仍存在争议。本研究旨在确定中国东北地区早产儿脐带血25-羟基维生素D [25(OH)D]评估的维生素D缺乏患病率,并评估25(OH)D预测BPD的能力及最佳阈值。
回顾性分析已知脐带血25(OH)D水平的VLBW和ELBW早产儿的临床资料。根据脐带血25(OH)D水平和BPD诊断将婴儿分组。进行逻辑回归以评估BPD的危险因素并建立列线图。采用受试者工作特征(ROC)曲线分析评估脐带血25(OH)D浓度预测BPD的最佳阈值。
共纳入267例早产儿,其中225例(84.3%)存在维生素D缺乏,134例(50.2%)被诊断为BPD。25(OH)D水平>20 ng/ml组的BPD发病率低于其他组(P = 0.024)。患BPD的婴儿脐带血25(OH)D水平低于未患BPD的婴儿(11.6 vs. 13.6 ng/ml,P = 0.016)。多因素逻辑回归模型显示,25(OH)D水平(比值比[OR]=0.933,95%置信区间[95%CI]:0.891-0.977)、胎龄(OR = 0.561,95%CI:0.425-0.740)、呼吸窘迫综合征(OR = 2.989,95%CI:1.455-6.142)和肺炎(OR = 2.546,95%CI:1.398-4.639)是BPD的独立危险因素。建立了包含这四个危险因素的预测列线图,其C指数为0.814。ROC曲线分析显示,预测BPD 的25(OH)D最佳截断值为15.7 ng/ml(曲线下面积 = 0.585,95%CI:0.523-0.645,P = 0.016),灵敏度为75.4%,特异度为42.9%。
脐带血25(OH)D水平<15.7 ng/ml对BPD的发生具有预测价值。本研究建立的列线图可帮助儿科医生更有效、更轻松地预测BPD风险。