Division of Medical Oncology, Pelotonia Institute for Immuno-Oncology, The Ohio State University Comprehensive Cancer Center, Columbus, OH, USA.
Stefanie Spielman Comprehensive Breast Center, Columbus, OH, USA.
J Hematol Oncol. 2022 Aug 28;15(1):118. doi: 10.1186/s13045-022-01335-y.
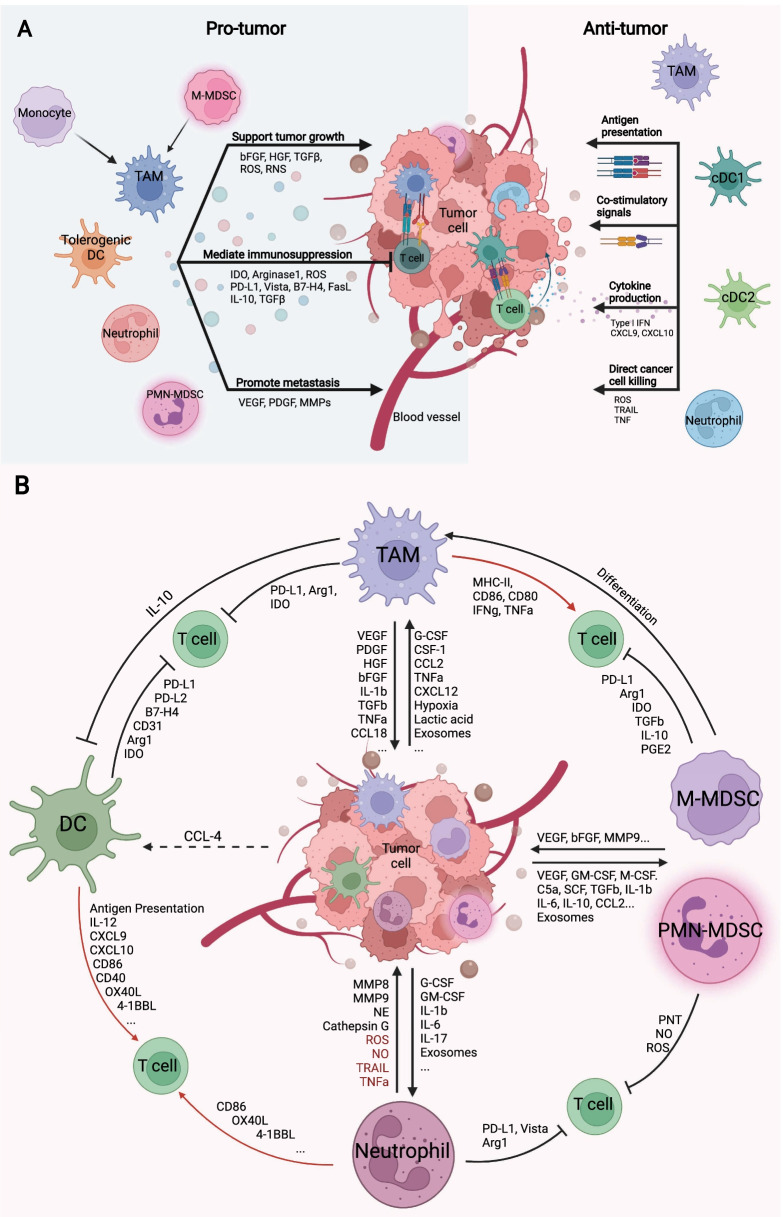
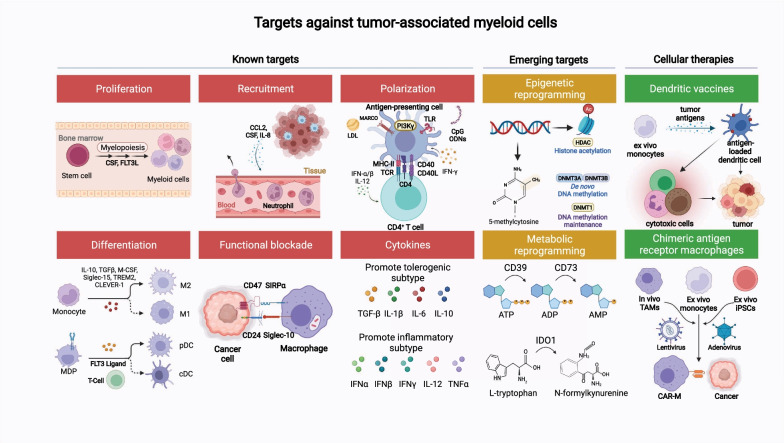
Immune checkpoint inhibitors targeting programmed cell death protein 1, programmed death-ligand 1, and cytotoxic T-lymphocyte-associated protein 4 provide deep and durable treatment responses which have revolutionized oncology. However, despite over 40% of cancer patients being eligible to receive immunotherapy, only 12% of patients gain benefit. A key to understanding what differentiates treatment response from non-response is better defining the role of the innate immune system in anti-tumor immunity and immune tolerance. Teleologically, myeloid cells, including macrophages, dendritic cells, monocytes, and neutrophils, initiate a response to invading pathogens and tissue repair after pathogen clearance is successfully accomplished. However, in the tumor microenvironment (TME), these innate cells are hijacked by the tumor cells and are imprinted to furthering tumor propagation and dissemination. Major advancements have been made in the field, especially related to the heterogeneity of myeloid cells and their function in the TME at the single cell level, a topic that has been highlighted by several recent international meetings including the 2021 China Cancer Immunotherapy workshop in Beijing. Here, we provide an up-to-date summary of the mechanisms by which major myeloid cells in the TME facilitate immunosuppression, enable tumor growth, foster tumor plasticity, and confer therapeutic resistance. We discuss ongoing strategies targeting the myeloid compartment in the preclinical and clinical settings which include: (1) altering myeloid cell composition within the TME; (2) functional blockade of immune-suppressive myeloid cells; (3) reprogramming myeloid cells to acquire pro-inflammatory properties; (4) modulating myeloid cells via cytokines; (5) myeloid cell therapies; and (6) emerging targets such as Siglec-15, TREM2, MARCO, LILRB2, and CLEVER-1. There is a significant promise that myeloid cell-based immunotherapy will help advance immuno-oncology in years to come.
针对程序性细胞死亡蛋白 1、程序性死亡配体 1 和细胞毒性 T 淋巴细胞相关蛋白 4 的免疫检查点抑制剂提供了深刻而持久的治疗反应,彻底改变了肿瘤学。然而,尽管超过 40%的癌症患者有资格接受免疫治疗,但只有 12%的患者受益。理解治疗反应与无反应的区别的关键是更好地定义先天免疫系统在抗肿瘤免疫和免疫耐受中的作用。从目的论上讲,髓样细胞,包括巨噬细胞、树突状细胞、单核细胞和中性粒细胞,在清除病原体后,会对入侵病原体和组织修复做出反应。然而,在肿瘤微环境(TME)中,这些先天细胞被肿瘤细胞劫持,并被印记以促进肿瘤的增殖和扩散。该领域取得了重大进展,特别是在髓样细胞的异质性及其在 TME 中的单细胞水平功能方面,这是最近包括 2021 年北京中国癌症免疫治疗研讨会在内的几次国际会议强调的主题。在这里,我们提供了最新的综述,总结了 TME 中的主要髓样细胞促进免疫抑制、促进肿瘤生长、促进肿瘤可塑性和赋予治疗耐药性的机制。我们讨论了针对临床前和临床环境中髓样细胞区室的正在进行的策略,包括:(1)改变 TME 中的髓样细胞组成;(2)功能性阻断免疫抑制性髓样细胞;(3)重新编程髓样细胞以获得促炎特性;(4)通过细胞因子调节髓样细胞;(5)髓样细胞治疗;(6)新兴靶点,如 Siglec-15、TREM2、MARCO、LILRB2 和 CLEVER-1。有很大的希望是,基于髓样细胞的免疫疗法将有助于在未来几年推进免疫肿瘤学。