VA HSR&D Center for Innovation to Implementation (Ci2i), VA Palo Alto Health Care System, Palo Alto, CA, USA.
School of Public Health, University of Nevada Reno, Reno, NV, USA.
J Gen Intern Med. 2022 Sep;37(Suppl 3):690-697. doi: 10.1007/s11606-022-07591-5. Epub 2022 Aug 30.
The Veterans Health Administration (VA) refers patients to community providers for specialty services not available on-site. However, community-level specialist shortages may impede access to care.
Compare gynecologist supply in veterans' county of residence versus at their VA site.
We identified women veteran VA patients from fiscal year (FY) 2017 administrative data and assessed availability of a VA gynecologist within 50 miles (hereafter called "local") of veterans' VA homesites (per national VA organizational survey data). For the same cohort, we then assessed community-level gynecologist availability; counties with < 2 gynecologists/10,000 women (per the Area Health Resource File) were "inadequate-supply" counties. We examined the proportion of women veterans with local VA gynecologist availability in counties with inadequate versus adequate gynecologist supply, stratified by individual and VA homesite characteristics. Chi-square tests assessed statistical differences.
All women veteran FY2017 VA primary care users nationally.
Availability of a VA gynecologist within 50 miles of a veteran's VA homesite; county-level "inadequate-supply" of gynecologists.
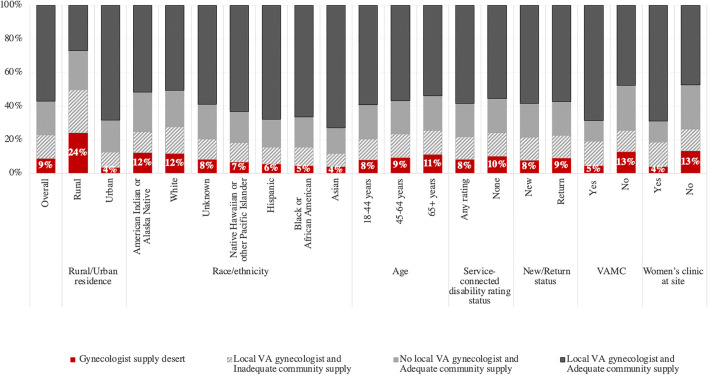
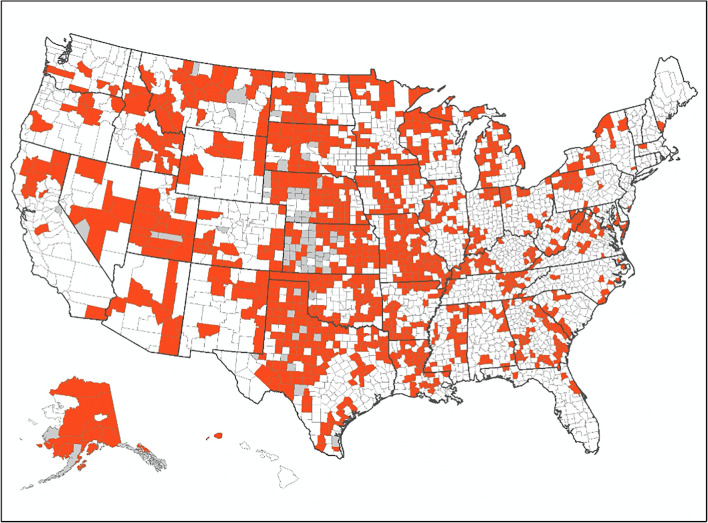
Among 407,482 women, 9% were in gynecologist supply deserts (i.e., lacking local VA gynecologist and living in an inadequate-supply county). The sub-populations with the highest proportions in gynecologist supply deserts were rural residents (24%), those who got their primary care at non-VAMC satellite clinics (13%), those who got their care at a site without a women's clinic (13%), and those with American Indian or Alaska Native (12%), or white (12%) race. Among those in inadequate-supply counties, 59.9% had gynecologists at their local VA; however, 40.1% lacked a local VA gynecologist.
Most veterans living in inadequate-supply counties had local VA gynecology care, reflecting VA's critical role as a safety net provider. However, for those in gynecologist supply deserts, expanded transportation options, modified staffing models, or tele-gynecology hubs may offer solutions to extend VA gynecology capacity.
退伍军人事务部(VA)将患者转介到社区医疗机构,以提供现场无法提供的专业服务。然而,社区层面的专家短缺可能会阻碍患者获得治疗。
比较退伍军人所在县的妇科医生供应情况与他们在 VA 地点的供应情况。
我们从 2017 财年(FY)的行政数据中确定了女性退伍军人 VA 患者,并评估了退伍军人 VA 住地 50 英里范围内 VA 妇科医生的可用性(根据全国 VA 组织调查数据)。对于同一队列,我们随后评估了社区层面的妇科医生供应情况;根据《地区卫生资源档案》,每 10000 名女性中有<2 名妇科医生的县为“供应不足”县。我们检查了在妇科医生供应不足和供应充足的县中,有当地 VA 妇科医生供应的女性退伍军人比例,按个人和 VA 住地特征进行分层。卡方检验评估了统计学差异。
全国范围内所有 2017 财年使用 VA 初级保健的女性退伍军人。
退伍军人 VA 住地 50 英里范围内 VA 妇科医生的可用性;县一级的妇科医生“供应不足”情况。
在 407482 名女性中,有 9%处于妇科医生供应荒漠地区(即缺乏当地 VA 妇科医生且居住在供应不足的县)。在妇科医生供应荒漠地区比例最高的亚人群是农村居民(24%)、在非 VA 卫星诊所接受初级保健的人群(13%)、在没有妇女诊所的地点接受保健的人群(13%)以及美国印第安人或阿拉斯加原住民(12%)或白人(12%)种族的人群。在供应不足的县中,59.9%的人在当地 VA 有妇科医生;然而,仍有 40.1%的人缺乏当地 VA 妇科医生。
大多数居住在供应不足的县的退伍军人在当地 VA 接受妇科保健,这反映了 VA 作为医疗保障提供者的重要作用。然而,对于那些处于妇科医生供应荒漠地区的人来说,扩大交通选择、修改人员配备模式或远程妇科医生中心可能是扩大 VA 妇科服务能力的解决方案。