Praxis für Interdisziplinäre Onkologie & Hämatologie, Freiburg, Germany.
Hämatologisch-Onkologische Praxis Eppendorf (HOPE), Hamburg, Germany.
Int J Cancer. 2023 Feb 1;152(3):458-469. doi: 10.1002/ijc.34271. Epub 2022 Sep 22.
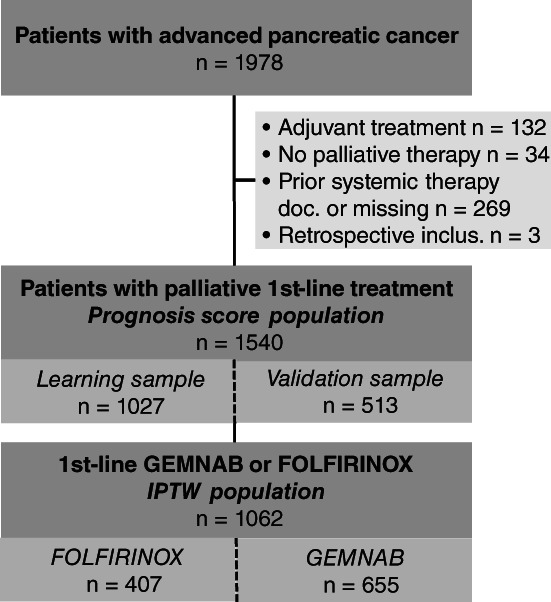
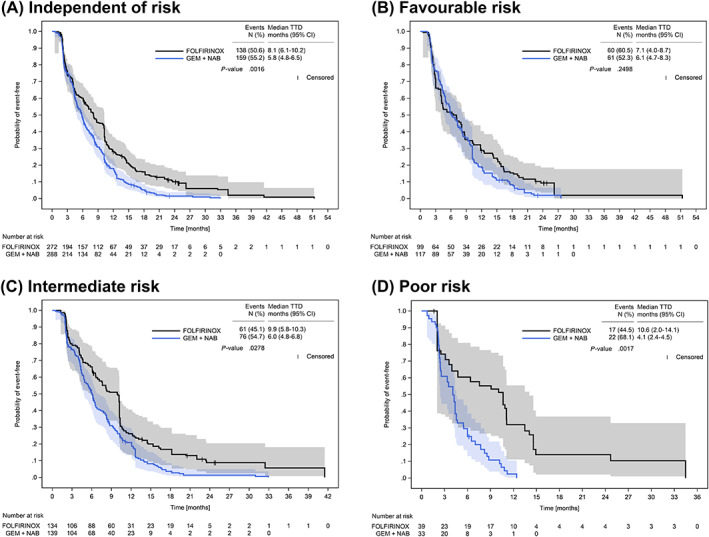
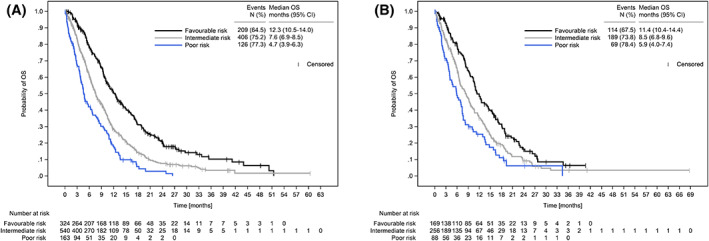
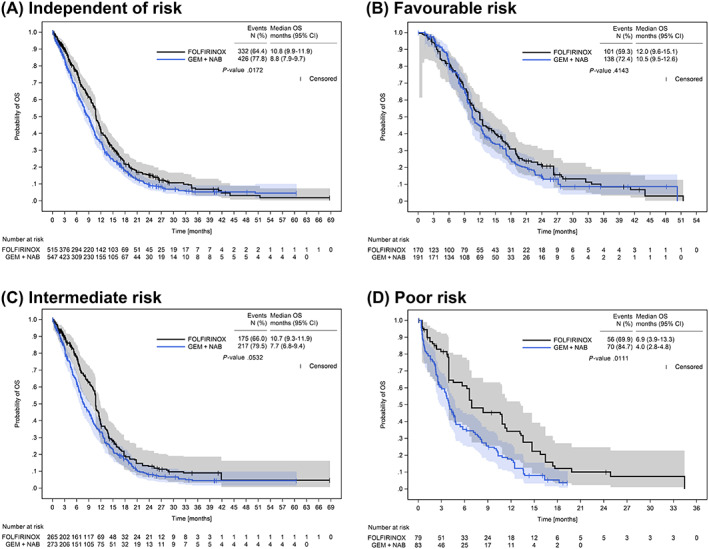
There is no prospective, randomised head-to-head trial comparing first-line FOLFIRINOX and gemcitabine/nab-paclitaxel in advanced pancreatic cancer. We assess real-world effectiveness and quality of life (QoL) of both regimens using a new prognostic score. This analysis includes 1540 patients with advanced pancreatic cancer from the prospective, clinical cohort study Tumour Registry Pancreatic Cancer separated into learning (n = 1027) and validation sample (n = 513). The Pancreatic Cancer Score (PCS) was developed using multivariate Cox regression. We compared overall survival (OS) and time to deterioration (TTD) for longitudinal QoL between first-line FOLFIRINOX (n = 407) and gemcitabine/nab-paclitaxel (n = 655) according to patients' prognostic risk, after inverse probability of treatment weighting (IPTW) by propensity score analysis. The PCS includes nine independent prognostic factors for survival: female sex, BMI ≥24/unknown, ECOG performance status ≥1, Charlson comorbidity index ≥1, tumour staging IV/unknown at primary diagnosis, liver metastases, bilirubin >1.5× upper limit of normal (ULN), leukocytes >ULN and neutrophil-to-lymphocyte ratio ≥4. Median OS of the validation sample was 11.4 (95% confidence interval [CI]: 10.4-14.4), 8.5 (95% CI: 6.8-9.6) and 5.9 months (95% CI: 4.0-7.4) for favourable- (0-3 risk factors), intermediate- (4-5 factors) and poor-risk group (6-9 factors), respectively. After IPTW, only poor-risk patients had significantly longer median OS and TTD of overall QoL with FOLFIRINOX (OS: 6.9 months, 95% CI: 3.9-13.3; TTD: 10.6 months, 95% CI: 2.0-14.1) vs gemcitabine/nab-paclitaxel (OS: 4.0 months, 95% CI: 2.8-4.8; TTD: 4.1 months, 95% CI: 2.4-4.5). Our novel PCS may facilitate treatment decisions in clinical routine of advanced pancreatic cancer, since only poor-risk, but not favourable-risk patients, seem to benefit from intensified treatment with FOLFIRINOX.
目前尚无头对头比较一线 FOLFIRINOX 方案和吉西他滨/白蛋白紫杉醇方案治疗晚期胰腺癌的前瞻性随机对照试验。我们使用新的预后评分来评估这两种方案的真实世界疗效和生活质量(QoL)。这项分析包括前瞻性临床队列研究肿瘤登记处胰腺癌中的 1540 名晚期胰腺癌患者,分为学习组(n=1027)和验证组(n=513)。使用多变量 Cox 回归开发了胰腺癌评分(PCS)。我们根据患者的预后风险,使用倾向评分分析的逆概率治疗加权(IPTW),比较了一线 FOLFIRINOX(n=407)和吉西他滨/白蛋白紫杉醇(n=655)治疗的总生存期(OS)和纵向 QoL 的恶化时间(TTD)。PCS 包括生存的 9 个独立预后因素:女性、BMI≥24/未知、ECOG 表现状态≥1、Charlson 合并症指数≥1、肿瘤分期在原发性诊断时为 IV/未知、肝转移、胆红素>1.5×正常值上限(ULN)、白细胞>ULN 和中性粒细胞与淋巴细胞比值≥4。验证组的中位 OS 分别为 11.4(95%置信区间[CI]:10.4-14.4)、8.5(95% CI:6.8-9.6)和 5.9 个月(95% CI:4.0-7.4),低危(0-3 个危险因素)、中危(4-5 个危险因素)和高危(6-9 个危险因素)组分别为。经过 IPTW 后,只有高危患者接受 FOLFIRINOX 治疗的中位 OS 和整体 QoL 的 TTD 显著延长(OS:6.9 个月,95%CI:3.9-13.3;TTD:10.6 个月,95%CI:2.0-14.1),而吉西他滨/白蛋白紫杉醇组为(OS:4.0 个月,95%CI:2.8-4.8;TTD:4.1 个月,95%CI:2.4-4.5)。我们的新 PCS 可能有助于在晚期胰腺癌的临床常规中做出治疗决策,因为只有高危患者,而不是低危患者,似乎从 FOLFIRINOX 的强化治疗中获益。