Division of Cardiology, Department of Internal Medicine Heart Vascular and Stroke Institute, Samsung Medical Center, Sungkyunkwan University School of Medicine Seoul Republic of Korea.
Department of Cardiology Keimyung University Dongsan Hospital Daegu Republic of Korea.
J Am Heart Assoc. 2022 Sep 20;11(18):e025956. doi: 10.1161/JAHA.122.025956. Epub 2022 Sep 8.
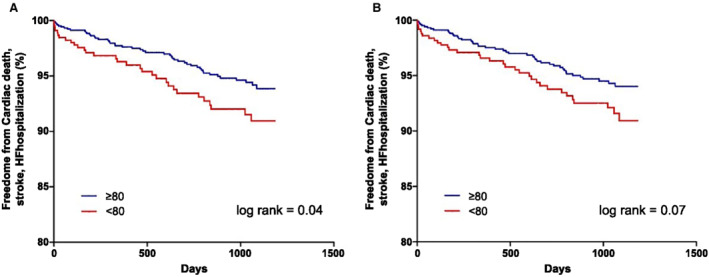
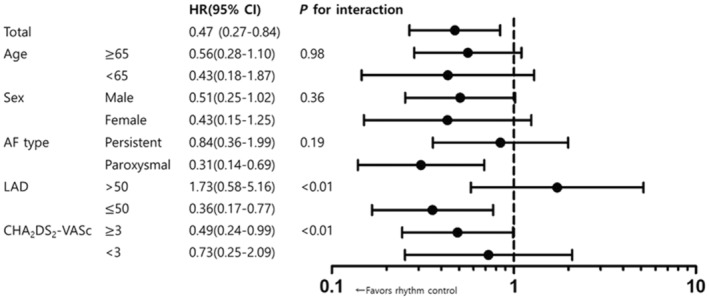
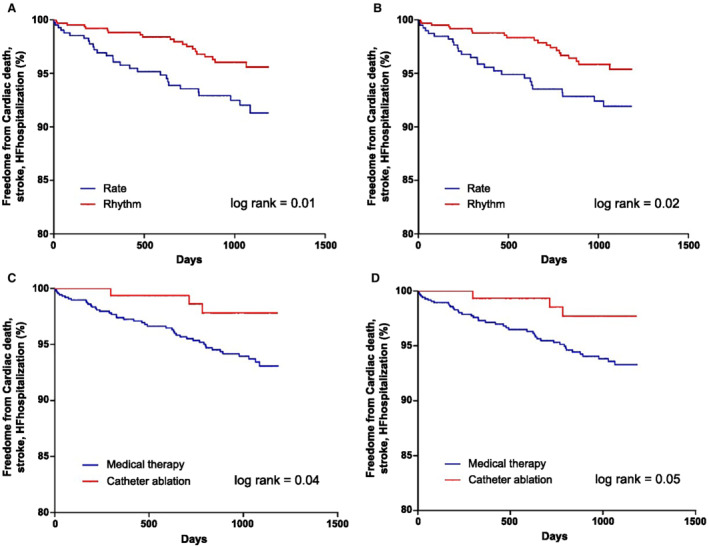
Background Atrial fibrillation (AF) is associated with an increased risk of poor cardiovascular outcomes; appropriate rhythm control can reduce the incidence of these adverse events. Therefore, catheter ablation is recommended in symptomatic patients with AF. The aims of this study were to compare AF-related outcomes according to a baseline symptom scale score and to determine the best treatment strategy for asymptomatic patients with AF. Methods and Results This study enrolled all patients who completed a baseline Atrial Fibrillation Effect on Quality-of-Life (AFEQT) survey in a prospective observational registry. The patients were divided into 2 groups according to AFEQT score at baseline; scores ≤80 were defined as symptomatic, whereas scores >80 represented asymptomatic patients. The primary outcome was defined as a composite of hospitalization for heart failure, ischemic stroke, or cardiac death. This study included 1515 patients (mean age: 65.7±10.5 years; 998 [65.9%] men). The survival curve showed a poorer outcome in the symptomatic group compared with the asymptomatic group (log-rank =0.04). Rhythm control led to a significantly lower risk of a composite outcome in asymptomatic patients (hazard ratio [HR], 0.47 [95% CI, 0.27-0.84], =0.01). Rhythm control was associated with more favorable composite outcomes in the asymptomatic group with paroxysmal AF, left atrium diameter ≤50 mm, and CHADS-VASc score ≥3. Conclusions Symptomatic patients with AF experienced more adverse outcomes compared with asymptomatic patients. In asymptomatic patients with AF, a strategy of rhythm control improved the outcomes, especially with paroxysmal AF, smaller left atrium size, or higher stroke risk. Registration URL: https://www.clinicaltrials.gov; Unique identifier: NCT02786095.
心房颤动(AF)与心血管不良结局风险增加相关;适当的节律控制可以降低这些不良事件的发生率。因此,建议对有症状的 AF 患者进行导管消融。本研究旨在根据基线症状量表评分比较 AF 相关结局,并确定无症状 AF 患者的最佳治疗策略。
本研究纳入了所有在前瞻性观察性登记中完成基线心房颤动对生活质量影响(AFEQT)调查的患者。根据基线 AFEQT 评分将患者分为 2 组;评分≤80 定义为有症状,评分>80 代表无症状患者。主要结局定义为心力衰竭、缺血性卒中和心脏死亡的复合住院。本研究纳入了 1515 例患者(平均年龄:65.7±10.5 岁;998 [65.9%] 为男性)。生存曲线显示,与无症状组相比,有症状组的结局较差(对数秩=0.04)。节律控制可显著降低无症状患者复合结局的风险(风险比 [HR],0.47 [95%CI,0.27-0.84],=0.01)。节律控制与无症状组阵发性 AF、左心房直径≤50mm 和 CHADS-VASc 评分≥3 的患者复合结局更有利相关。
与无症状患者相比,有症状的 AF 患者经历了更多的不良结局。在无症状的 AF 患者中,节律控制策略改善了结局,特别是在阵发性 AF、左心房较小或卒中风险较高的患者中。