Di Paola Valerio, Mazzotta Giorgio, Pignatelli Vincenza, Bufi Enida, D'Angelo Anna, Conti Marco, Panico Camilla, Fiorentino Vincenzo, Pierconti Francesco, Kilburn-Toppin Fleur, Belli Paolo, Manfredi Riccardo
Department of Bioimaging, Radiation Oncology and Hematology, UOC of Radiologia, Fondazione Policlinico Universitario A. Gemelli IRCSS, Largo A. Gemelli 8, 00168 Rome, Italy.
Institute of Radiology, Catholic University of the Sacred Heart, Largo A. Gemelli 8, 00168 Rome, Italy.
Cancers (Basel). 2022 Aug 31;14(17):4270. doi: 10.3390/cancers14174270.
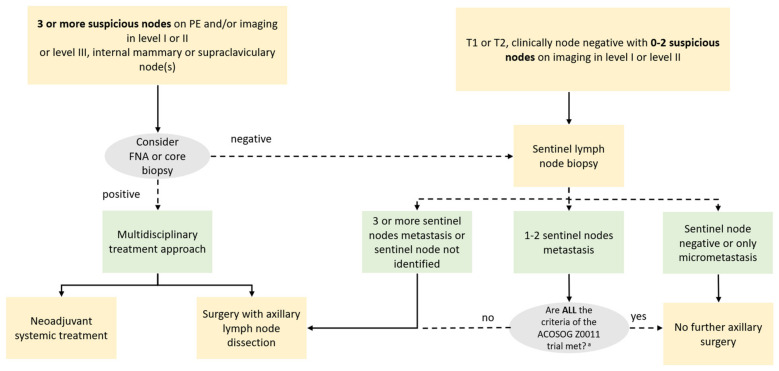
The correct N-staging in breast cancer is crucial to tailor treatment and stratify the prognosis. N-staging is based on the number and the localization of suspicious regional nodes on physical examination and/or imaging. Since clinical examination of the axillary cavity is associated with a high false negative rate, imaging modalities play a central role. In the presence of a T1 or T2 tumor and 0-2 suspicious nodes, on imaging at the axillary level I or II, a patient should undergo sentinel lymph node biopsy (SLNB), whereas in the presence of three or more suspicious nodes at the axillary level I or II confirmed by biopsy, they should undergo axillary lymph node dissection (ALND) or neoadjuvant chemotherapy according to a multidisciplinary approach, as well as in the case of internal mammary, supraclavicular, or level III axillary involved lymph nodes. In this scenario, radiological assessment of lymph nodes at the time of diagnosis must be accurate. False positives may preclude a sentinel lymph node in an otherwise eligible woman; in contrast, false negatives may lead to an unnecessary SLNB and the need for a second surgical procedure. In this review, we aim to describe the anatomy of the axilla and breast regional lymph node, and their diagnostic features to discriminate between normal and pathological nodes at Ultrasound (US) and Magnetic Resonance Imaging (MRI). Moreover, the technical aspects, the advantage and limitations of MRI versus US, and the possible future perspectives are also analyzed, through the analysis of the recent literature.
乳腺癌准确的N分期对于制定个体化治疗方案和判断预后分层至关重要。N分期基于体格检查和/或影像学检查中可疑区域淋巴结的数量和位置。由于腋窝临床检查的假阴性率较高,影像学检查方法起着核心作用。对于T1或T2期肿瘤且腋窝I或II级水平有0至2个可疑淋巴结的患者,经腋窝水平I或II级的影像学检查发现后,应进行前哨淋巴结活检(SLNB);而对于经活检证实腋窝I或II级水平有三个或更多可疑淋巴结的患者,应根据多学科方法进行腋窝淋巴结清扫(ALND)或新辅助化疗,对于内乳、锁骨上或腋窝III级受累淋巴结的情况同样如此。在这种情况下,诊断时对淋巴结的影像学评估必须准确。假阳性可能会使原本符合条件的女性无法进行前哨淋巴结活检;相反,假阴性可能导致不必要的前哨淋巴结活检以及需要进行二次手术。在本综述中,我们旨在描述腋窝和乳腺区域淋巴结的解剖结构,以及它们在超声(US)和磁共振成像(MRI)下区分正常和病理性淋巴结的诊断特征。此外,通过对近期文献的分析,还分析了MRI与US的技术方面、优势和局限性以及可能的未来前景。