Taweevisit Mana, Chindamporn Ariya, Sujjavorakul Kritsaporn, Samransamruajkit Rujipat, Thorner Paul Scott
Department of Pathology, Faculty of Medicine, Chulalongkorn University, Bangkok 10330, Thailand; King Chulalongkorn Memorial Hospital and Thai Red Cross Society, Bangkok 10330 Thailand.
King Chulalongkorn Memorial Hospital and Thai Red Cross Society, Bangkok 10330 Thailand; Department of Microbiology, Faculty of Medicine, Chulalongkorn University, Bangkok 10330, Thailand.
Pathol Res Pract. 2022 Oct;238:154106. doi: 10.1016/j.prp.2022.154106. Epub 2022 Sep 5.
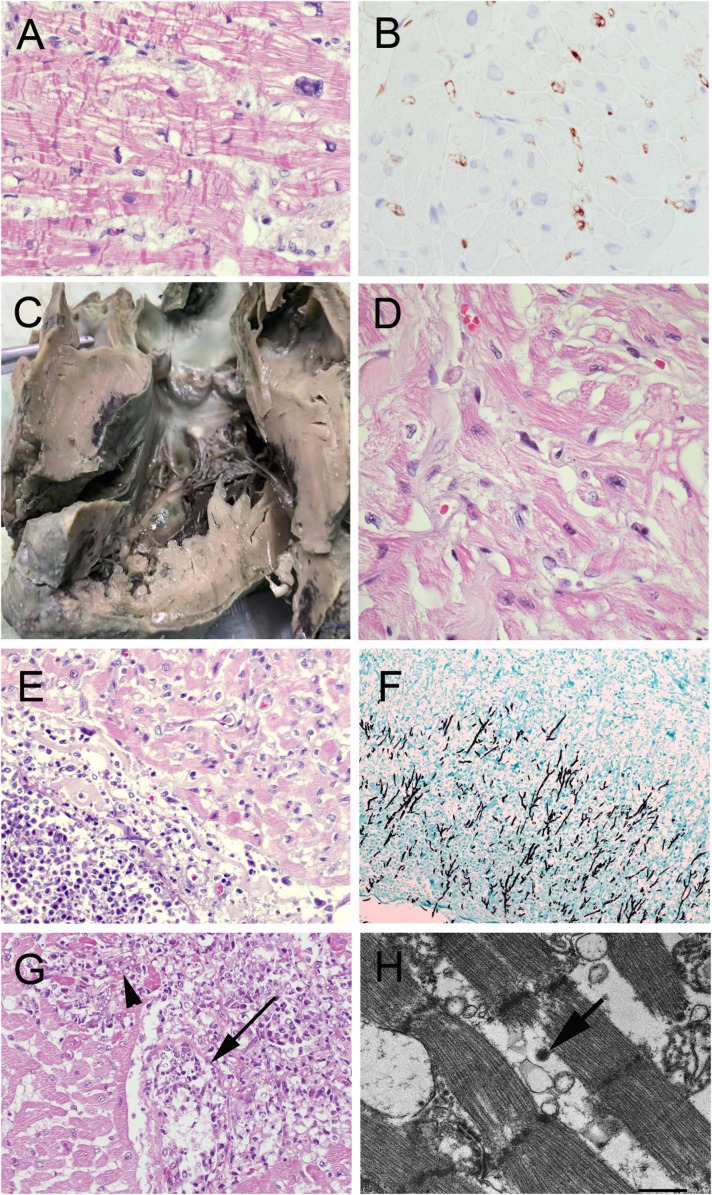
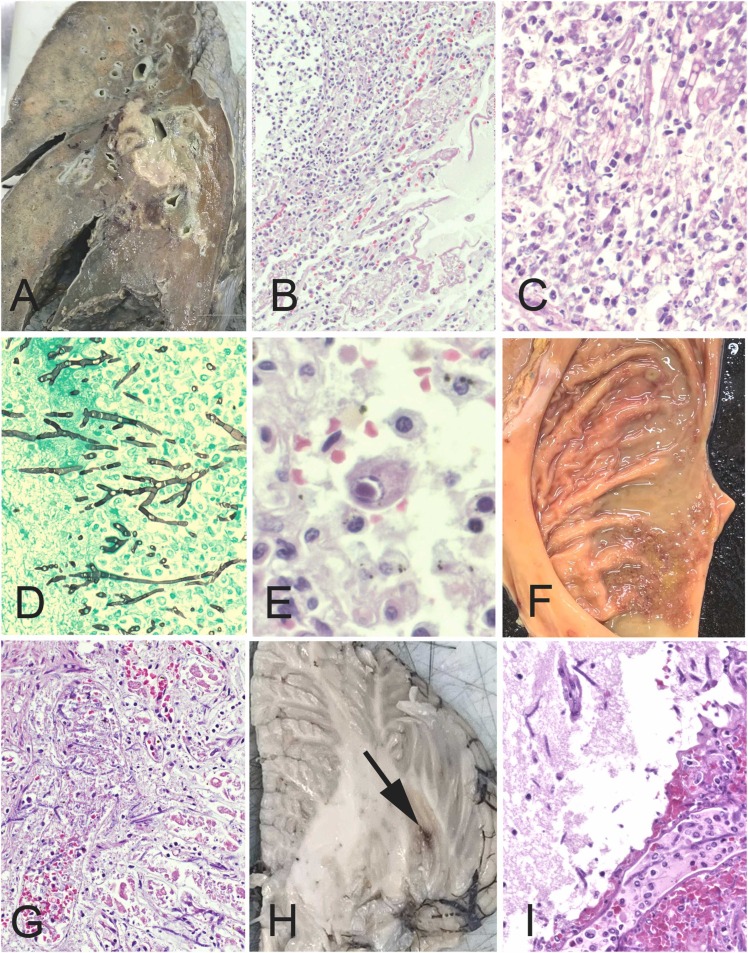
Multisystem inflammatory syndrome in children (MIS-C) is an emerging phenomenon associated with SARS-COV-2 infection (COVID-19) occurring in < 1 % of infected children. MIS-C is characterized by a hyperinflammatory state with excessive cytokine release ('storm') leading to hemodynamic compromise and multiorgan failure, with a death rate of ∼2 %. Autopsy examination can play a particularly important role in helping to understand the pathogenesis of MIS-C. Yet, only five autopsy studies have been reported to date. We report a fatal case of MIS-C involving a previously healthy, 5-year-old Thai boy admitted with MIS-C, one month after exposure to SARS-COV-2. While in intensive care, he was found to have a hypertrophic cardiomyopathy, and despite immunosuppressive treatment for MIS-C, developed shock and died. Multiorgan inflammation was not found at autopsy, implying that the MIS-C had responded to treatment. However, there was disseminated aspergillosis and cytomegalovirus reactivation, attributed to the immunosuppression. SARS-COV-2 virus was also found in multiple organs. To the best of our knowledge, this is the first reported autopsy of an MIS-C patient from Asia, and the first report of aspergillosis in MIS-C. This case underscores that the risks of immunosuppression are also a concern in MIS-C. Although MIS-C is generally considered to be a post-infectious hyperimmune reaction, persistence of SARS-COV-2 is a feature in all autopsies of MIS-C patients reported to date, suggesting a possible role in the pathogenesis, at least in fatal cases.
儿童多系统炎症综合征(MIS-C)是一种与严重急性呼吸综合征冠状病毒2(SARS-CoV-2)感染(新冠病毒病)相关的新出现现象,在<1%的感染儿童中发生。MIS-C的特征是炎症反应过度,细胞因子过度释放(“风暴”),导致血流动力学不稳定和多器官功能衰竭,死亡率约为2%。尸检在帮助理解MIS-C的发病机制方面可发挥特别重要的作用。然而,迄今为止仅报道了五项尸检研究。我们报告一例MIS-C致死病例,患者为一名5岁泰国男童,此前健康,接触SARS-CoV-2一个月后因MIS-C入院。在重症监护期间,发现他患有肥厚型心肌病,尽管接受了针对MIS-C的免疫抑制治疗,但仍发生休克并死亡。尸检未发现多器官炎症,这意味着MIS-C对治疗有反应。然而,存在播散性曲霉病和巨细胞病毒再激活,归因于免疫抑制。在多个器官中也发现了SARS-CoV-2病毒。据我们所知,这是亚洲首例报道的MIS-C患者尸检,也是MIS-C中曲霉病的首例报道。该病例强调免疫抑制的风险在MIS-C中也是一个值得关注的问题。尽管MIS-C通常被认为是一种感染后超免疫反应,但SARS-CoV-2的持续存在是迄今为止报道的所有MIS-C患者尸检中的一个特征,这表明其在发病机制中可能起作用,至少在致死病例中如此。