Academic Unit of Gastroenterology, Royal Hallamshire Hospital, Sheffield Teaching Hospital NHS Foundation Trust, Sheffield, UK.
Division of Nutritional Sciences, School of Biosciences, University of Nottingham, Nottingham, UK.
BMC Med. 2022 Sep 13;20(1):287. doi: 10.1186/s12916-022-02496-w.
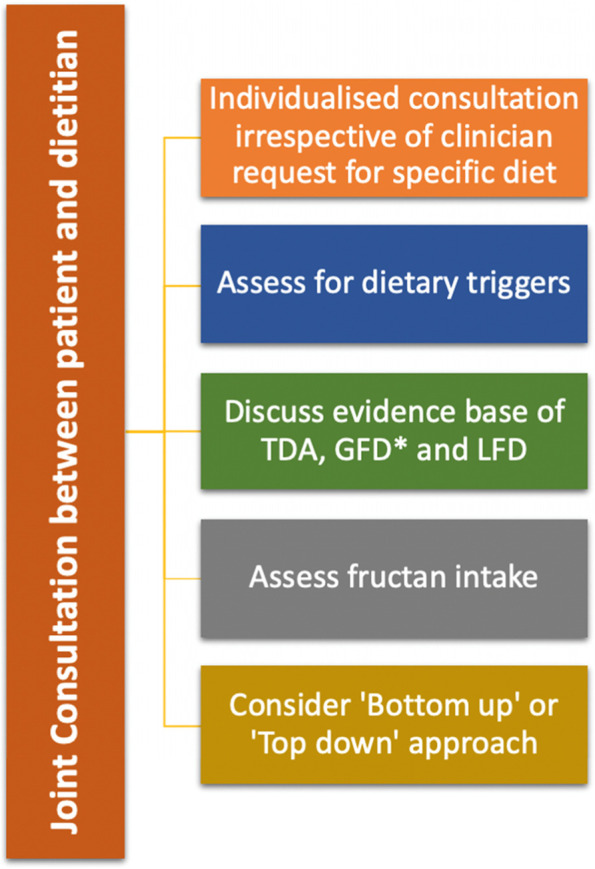
There has been a renewed interest in the role of dietary therapies to manage irritable bowel syndrome (IBS), with diet high on the agenda for patients. Currently, interest has focussed on the use of traditional dietary advice (TDA), a gluten-free diet (GFD) and the low FODMAP diet (LFD). A consensus meeting was held to assess the role of these dietary therapies in IBS, in Sheffield, United Kingdom.Evidence for TDA is from case control studies and clinical experience. Randomised controlled trials (RCT) have demonstrated the benefit of soluble fibre in IBS. No studies have assessed TDA in comparison to a habitual or sham diet. There have been a number of RCTs demonstrating the efficacy of a GFD at short-term follow-up, with a lack of long-term outcomes. Whilst gluten may lead to symptom generation in IBS, other components of wheat may also play an important role, with recent interest in the role of fructans, wheat germ agglutinins, as well as alpha amylase trypsin inhibitors. There is good evidence for the use of a LFD at short-term follow-up, with emerging evidence demonstrating its efficacy at long-term follow-up. There is overlap between the LFD and GFD with IBS patients self-initiating gluten or wheat reduction as part of their LFD. Currently, there is a lack of evidence to suggest superiority of one diet over another, although TDA is more acceptable to patients.In view of this evidence, our consensus group recommends that dietary therapies for IBS should be offered by dietitians who first assess dietary triggers and then tailor the intervention according to patient choice. Given the lack of dietetic services, novel approaches such as employing group clinics and online webinars may maximise capacity and accessibility for patients. Further research is also required to assess the comparative efficacy of dietary therapies to other management strategies available to manage IBS.
人们对饮食疗法在管理肠易激综合征 (IBS) 中的作用重新产生了兴趣,饮食成为患者关注的重点。目前,人们对传统饮食建议 (TDA)、无麸质饮食 (GFD) 和低 FODMAP 饮食 (LFD) 的兴趣日益浓厚。在英国谢菲尔德举行了一次共识会议,以评估这些饮食疗法在 IBS 中的作用。TDA 的证据来自病例对照研究和临床经验。随机对照试验 (RCT) 已经证明了可溶性纤维在 IBS 中的益处。没有研究将 TDA 与习惯性或模拟饮食进行比较。有许多 RCT 证明了 GFD 在短期随访中的疗效,但缺乏长期结果。虽然麸质可能导致 IBS 症状产生,但小麦的其他成分也可能发挥重要作用,最近人们对果聚糖、麦胚凝集素以及α-淀粉酶抑制剂的作用产生了兴趣。在短期随访中,LFD 的使用有很好的证据,新的证据表明其在长期随访中的疗效。LFD 和 GFD 之间存在重叠,IBS 患者自行减少麸质或小麦摄入量作为其 LFD 的一部分。目前,缺乏证据表明一种饮食优于另一种饮食,尽管 TDA 更受患者接受。鉴于这一证据,我们的共识小组建议,营养师应向 IBS 患者提供饮食疗法,营养师首先评估饮食诱因,然后根据患者的选择调整干预措施。鉴于饮食服务的缺乏,采用小组诊所和在线网络研讨会等新方法可能会最大限度地提高患者的容量和可及性。还需要进一步研究来评估饮食疗法与其他可用于管理 IBS 的管理策略相比的相对疗效。