Division of Gastroenterology and Hepatology, Perelman School of Medicine, University of Pennsylvania, Philadelphia.
Department of Medicine, Corporal Michael J. Crescenz VA Medical Center, Philadelphia, Pennsylvania.
JAMA Netw Open. 2022 Sep 1;5(9):e2231601. doi: 10.1001/jamanetworkopen.2022.31601.
Patients with cirrhosis have increased risk of postoperative mortality. Several models have been developed to estimate this risk; however, current risk estimation scores cannot compare surgical risk with the risk of not operating.
To identify clinical optimal thresholds to favor operative or nonoperative management for a common cirrhosis surgical scenario, the symptomatic abdominal hernia.
DESIGN, SETTING, AND PARTICIPANTS: This was a Markov cohort decision analytical modeling study evaluating elective surgery vs nonoperative management for a symptomatic abdominal hernia in a patient with cirrhosis. Transition probabilities and utilities were derived from the literature and from data using an established cirrhosis cohort in the Veterans Health Administration. Participants included patients who were referred to a surgery clinic for a symptomatic abdominal hernia. Data were obtained from patients diagnosed with cirrhosis between January 1, 2008 and December 31, 2018. Data were analyzed from January 1 to May 1, 2022.
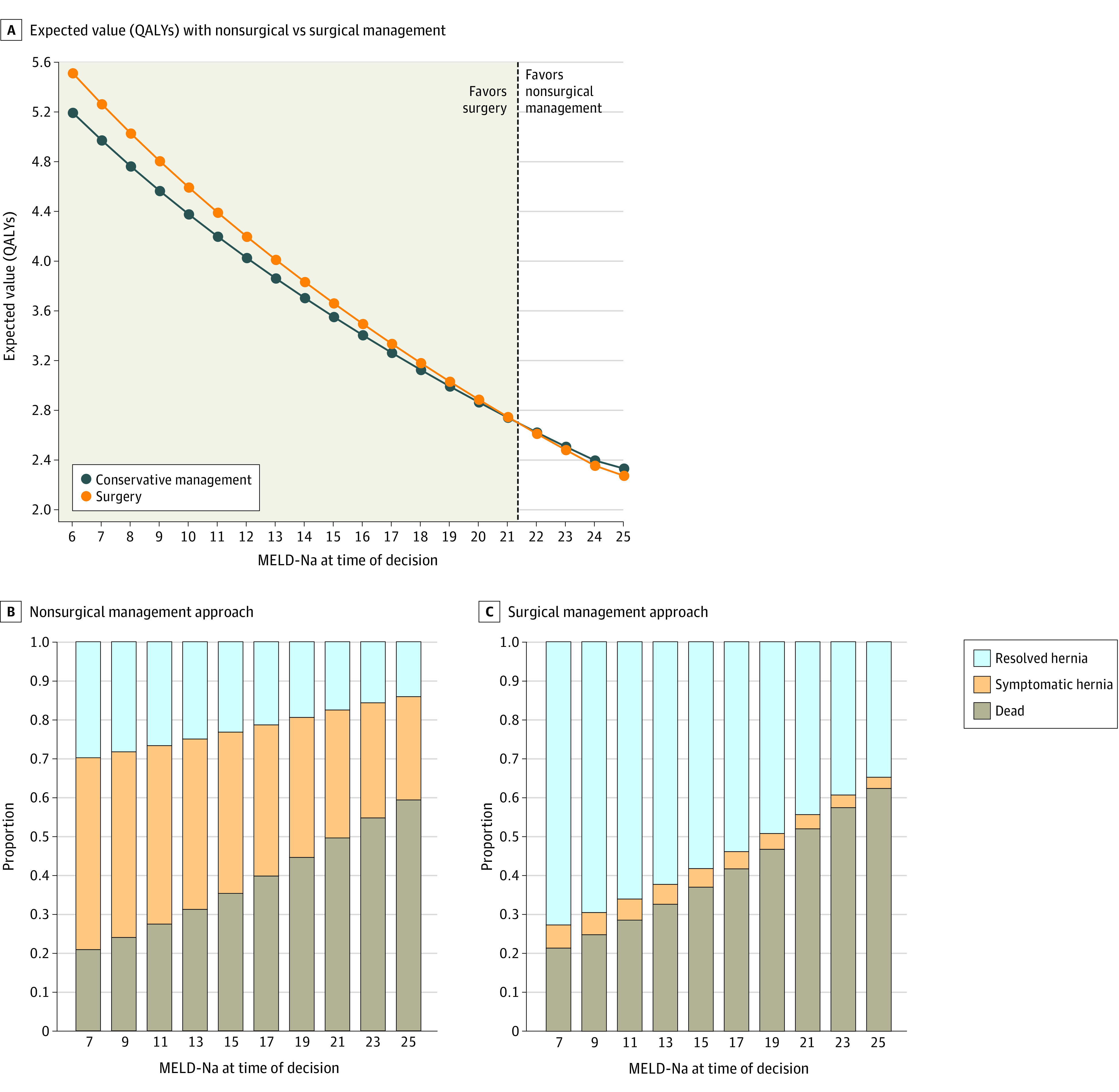
Expected quality-adjusted life-years (QALYs) were estimated for each pathway and iterated over baseline model for end-stage liver disease-sodium (MELD-Na) scores ranging from 6 to 25. Markov models were cycled over a 5-year time horizon.
A total 2740 patients with cirrhosis (median [IQR] age, 62 [56-66] years; 2699 [98.5%] men) were referred to a surgery clinic for a symptomatic abdominal hernia; 1752 patients (63.9%) did not receive surgery. The median (IQR) follow-up was 42.1 (25.3-70.0) months. Using this cohort to estimate the mortality risk of operative and nonoperative pathways, an initial MELD-Na threshold of 21.3 points, below which surgery was associated with maximized QALYs was identified. Nonoperative management was associated with increased QALYs above this MELD-Na threshold. Although more patients experienced death with a surgical treatment decision across all initial MELD-Na values, this was counterbalanced by increased time spent in a resolved hernia state associated with increased utility. Model results were sensitive to the probability of hernia recurrence and hernia incarceration and utility decrement in the symptomatic hernia state.
This decision analytical model study found that elective surgical treatment for a symptomatic abdominal hernia was favored even in the setting of relatively high MELD-Na scores. Patient symptoms, hernia-specific characteristics, and surgeon and center expertise may potentially impact the optimal strategy, emphasizing the importance of shared decision-making.
患有肝硬化的患者术后死亡率增加。已经开发了几种模型来估计这种风险;然而,目前的风险评估评分不能将手术风险与不手术的风险进行比较。
确定临床最佳阈值,以有利于肝硬化常见手术情况,即症状性腹部疝的手术或非手术治疗。
设计、设置和参与者:这是一项马尔可夫队列决策分析模型研究,评估了对肝硬化患者症状性腹部疝进行择期手术与非手术治疗的情况。转移概率和效用来自文献和使用退伍军人健康管理局中已建立的肝硬化队列的数据。参与者包括因症状性腹部疝而被转介到手术诊所的患者。数据来自 2008 年 1 月 1 日至 2018 年 12 月 31 日期间被诊断为肝硬化的患者。数据于 2022 年 1 月 1 日至 5 月 1 日进行分析。
为每个路径估计了预期的质量调整生命年(QALY),并对终末期肝病钠(MELD-Na)评分从 6 到 25 的基线模型进行了迭代。马尔可夫模型在 5 年的时间范围内循环。
共有 2740 名肝硬化患者(中位[IQR]年龄,62[56-66]岁;2699[98.5%]男性)因症状性腹部疝被转介至手术诊所;1752 名患者(63.9%)未接受手术。中位(IQR)随访时间为 42.1(25.3-70.0)个月。使用该队列估计手术和非手术途径的死亡率风险,确定了初始 MELD-Na 阈值为 21.3 分,低于该阈值,手术与最大化 QALY 相关。在这个 MELD-Na 阈值以上,非手术治疗与增加的 QALY 相关。尽管在所有初始 MELD-Na 值下,手术治疗决策都会导致更多患者死亡,但这被与增加的效用相关的疝状态的解决时间增加所抵消。模型结果对疝复发和疝嵌顿的概率以及症状性疝状态下的疝效用下降敏感。
这项决策分析模型研究发现,即使在相对较高的 MELD-Na 评分下,对症状性腹部疝进行择期手术治疗也是有利的。患者症状、疝的具体特征以及外科医生和中心的专业知识可能会影响最佳策略,强调了共同决策的重要性。