Center for Computational Medicine in Cardiology, Università della Svizzera Italiana, Lugano, Switzerland.
Maria Cecilia Hospital, GVM Care and Research, Cotignola, Italy.
Europace. 2023 Feb 16;25(2):546-553. doi: 10.1093/europace/euac157.
Electromechanical coupling in patients receiving cardiac resynchronization therapy (CRT) is not fully understood. Our aim was to determine the best combination of electrical and mechanical substrates associated with effective CRT.
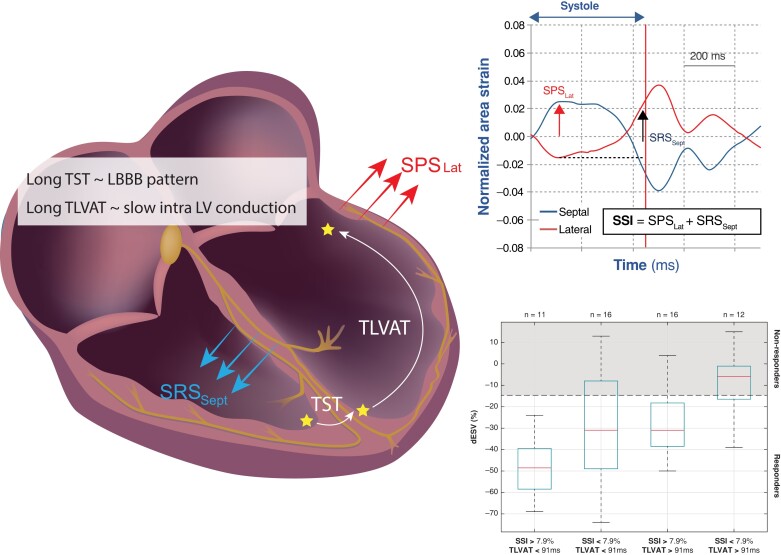
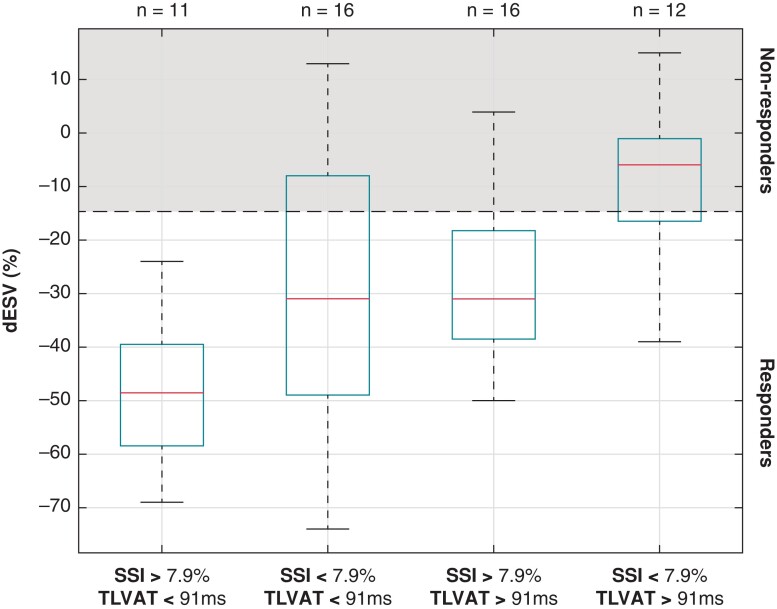
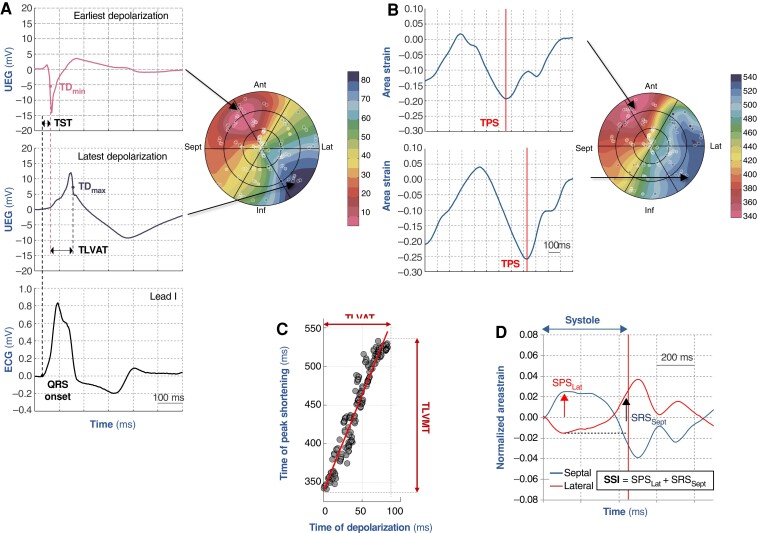
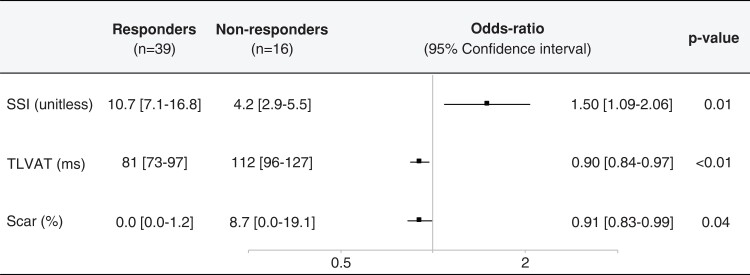
Sixty-two patients were prospectively enrolled from two centres. Patients underwent 12-lead electrocardiogram (ECG), cardiovascular magnetic resonance (CMR), echocardiography, and anatomo-electromechanical mapping (AEMM). Remodelling was measured as the end-systolic volume (ΔESV) decrease at 6 months. CRT was defined effective with ΔESV ≤ -15%. QRS duration (QRSd) was measured from ECG. Area strain was obtained from AEMM and used to derive systolic stretch index (SSI) and total left-ventricular mechanical time. Total left-ventricular activation time (TLVAT) and transeptal time (TST) were derived from AEMM and ECG. Scar was measured from CMR. Significant correlations were observed between ΔESV and TST [rho = 0.42; responder: 50 (20-58) vs. non-responder: 33 (8-44) ms], TLVAT [-0.68; 81 (73-97) vs. 112 (96-127) ms], scar [-0.27; 0.0 (0.0-1.2) vs. 8.7 (0.0-19.1)%], and SSI [0.41; 10.7 (7.1-16.8) vs. 4.2 (2.9-5.5)], but not QRSd [-0.13; 155 (140-176) vs. 167 (155-177) ms]. TLVAT and SSI were highly accurate in identifying CRT response [area under the curve (AUC) > 0.80], followed by scar (AUC > 0.70). Total left-ventricular activation time (odds ratio = 0.91), scar (0.94), and SSI (1.29) were independent factors associated with effective CRT. Subjects with SSI >7.9% and TLVAT <91 ms all responded to CRT with a median ΔESV ≈ -50%, while low SSI and prolonged TLVAT were more common in non-responders (ΔESV ≈ -5%).
Electromechanical measurements are better associated with CRT response than conventional ECG variables. The absence of scar combined with high SSI and low TLVAT ensures effectiveness of CRT.
心脏再同步治疗(CRT)患者的机电耦联尚不完全清楚。我们的目的是确定与有效 CRT 相关的最佳电和机械底物组合。
前瞻性纳入来自两个中心的 62 例患者。患者接受 12 导联心电图(ECG)、心血管磁共振(CMR)、超声心动图和解剖机电映射(AEMM)检查。以 6 个月时的左室收缩末期容积(ΔESV)减少来衡量重构。ΔESV ≤-15%定义为 CRT 有效。QRS 时限(QRSd)从心电图测量。AEMM 获得的面积应变用于得出收缩期拉伸指数(SSI)和总左室机械时间。从 AEMM 和心电图得出总左室激活时间(TLVAT)和穿隔时间(TST)。CMR 测量瘢痕。ΔESV 与 TST 呈显著相关[rho=0.42;应答者:50(20-58)vs. 非应答者:33(8-44)ms],TLVAT[-0.68;81(73-97)vs. 112(96-127)ms],瘢痕[-0.27;0.0(0.0-1.2)vs. 8.7(0.0-19.1)%],SSI [0.41;10.7(7.1-16.8)vs. 4.2(2.9-5.5)],但 QRSd 无相关性[-0.13;155(140-176)vs. 167(155-177)ms]。TLVAT 和 SSI 对识别 CRT 反应的准确性较高(曲线下面积(AUC)>0.80),其次是瘢痕(AUC>0.70)。总左室激活时间(比值比=0.91)、瘢痕(0.94)和 SSI(1.29)是与有效 CRT 相关的独立因素。SSI>7.9%和 TLVAT<91ms 的患者 CRT 后 ΔESV 中位数约为-50%,而低 SSI 和长 TLVAT 更常见于无应答者(ΔESV 约为-5%)。
与传统 ECG 变量相比,机电测量与 CRT 反应相关性更好。不存在瘢痕,同时 SSI 高和 TLVAT 低可确保 CRT 的有效性。