Department of Atherosclerosis, Instituto do Coração (InCor), Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo, São Paulo, São Paulo, Brazil.
Heart and Stroke/Richard Lewar Centres of Excellence in Cardiovascular Research, Peter Munk Cardiac Centre, University of Toronto, Toronto, Ontario, Canada.
BMJ Open. 2022 Sep 22;12(9):e062378. doi: 10.1136/bmjopen-2022-062378.
Coronary atherosclerotic burden and SYNTAX Score (SS) are predictors of cardiovascular events.
To investigate the value of SYNTAX scores (SS, SYNTAX Score II (SSII) and residual SYNTAX Score (rSS)) for predicting cardiovascular events in patients with coronary artery disease (CAD).
Retrospective cohort study.
Single tertiary centre.
Medicine, Angioplasty or Surgery Study database patients with stable multivessel CAD and preserved ejection fraction.
Patients with CAD undergoing coronary artery bypass graft (CABG), percutaneous coronary intervention (PCI) or medical treatment (MT) alone from January 2002 to December 2015.
Primary: 5-year all-cause mortality. Secondary: composite of all-cause death, myocardial infarction, stroke and subsequent coronary revascularisation at 5 years.
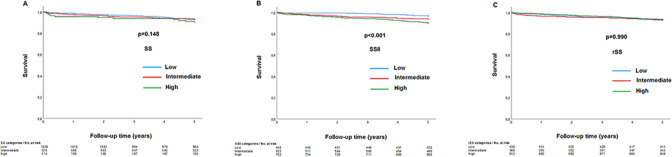
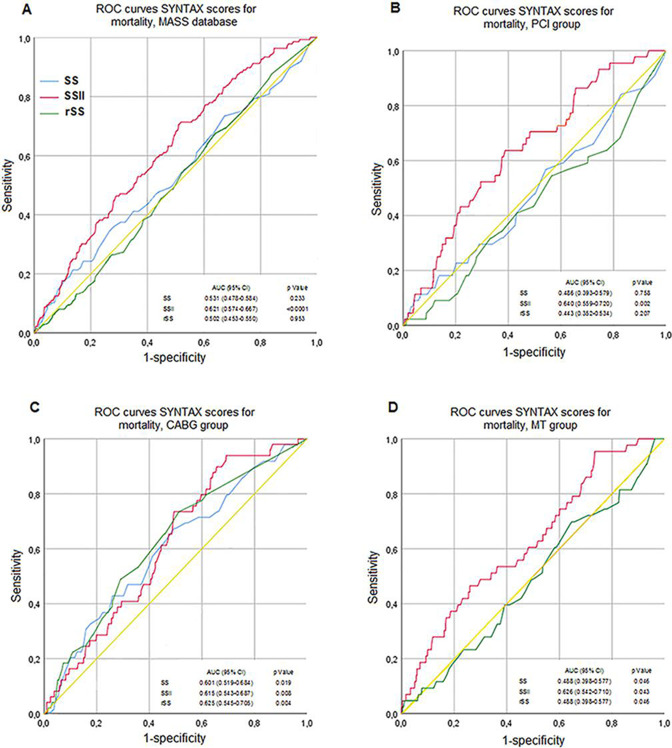
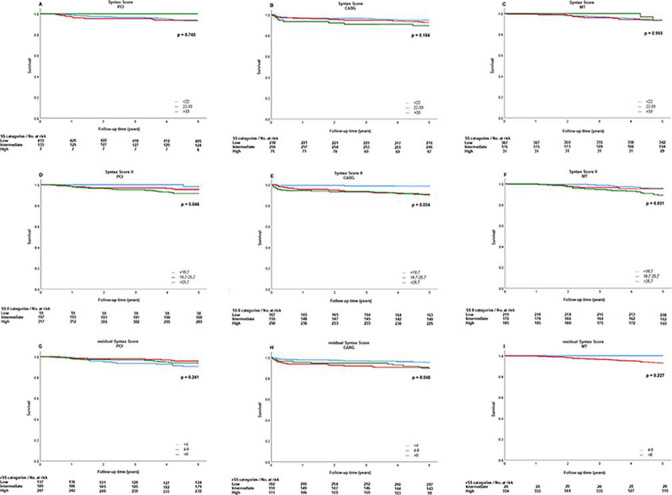
A total of 1719 patients underwent PCI (n=573), CABG (n=572) or MT (n=574) alone. The SS was not considered an independent predictor of 5-year mortality in the PCI (low, intermediate and high SS at 6.5%, 6.8% and 4.3%, respectively, p=0.745), CABG (low, intermediate and high SS at 5.7%, 8.0% and 12.1%, respectively, p=0.194) and MT (low, intermediate and high SS at 6.8%, 6.9% and 6.5%, respectively, p=0.993) cohorts. The SSII (low, intermediate and high SSII at 3.6% vs 7.9% vs 10.5%, respectively, p<0.001) was associated with a higher mortality risk in the overall population. Within each treatment strategy, SSII was associated with a significant 5-year mortality rate, especially in CABG patients with higher SSII (low, intermediate and high SSII at 1.8%, 9.7% and 10.0%, respectively, p=0.004) and in MT patients with high SSII (low, intermediate and high SSII at 5.0%, 4.7% and 10.8%, respectively, p=0.031). SSII demonstrated a better predictive accuracy for mortality compared with SS and rSS (c-index=0.62).
Coronary atherosclerotic burden alone was not associated with significantly increased risk of all-cause mortality. The SSII better discriminates the risk of death.
ISRCTN66068876.
冠状动脉粥样硬化负担和 SYNTAX 评分(SS)是心血管事件的预测因子。
探讨 SYNTAX 评分(SS、SYNTAX Score II(SSII)和残余 SYNTAX 评分(rSS))在预测冠状动脉疾病(CAD)患者心血管事件中的价值。
回顾性队列研究。
单中心三级医院。
稳定多血管 CAD 和射血分数保留的患者的医学、血管成形术或手术研究数据库。
2002 年 1 月至 2015 年 12 月接受冠状动脉旁路移植术(CABG)、经皮冠状动脉介入治疗(PCI)或单独药物治疗(MT)的 CAD 患者。
主要结局:5 年全因死亡率。次要结局:5 年内全因死亡、心肌梗死、卒中和随后的冠状动脉血运重建的复合终点。
共有 1719 名患者接受了 PCI(n=573)、CABG(n=572)或 MT(n=574)治疗。在 PCI 患者中,SS 并不是 5 年死亡率的独立预测因素(低、中、高 SS 分别为 6.5%、6.8%和 4.3%,p=0.745)、CABG(低、中、高 SS 分别为 5.7%、8.0%和 12.1%,p=0.194)和 MT(低、中、高 SS 分别为 6.8%、6.9%和 6.5%,p=0.993)。SSII(低、中、高 SSII 分别为 3.6%、7.9%和 10.5%,p<0.001)与全人群的死亡率风险增加相关。在每种治疗策略中,SSII 与显著的 5 年死亡率相关,尤其是在 SSII 较高的 CABG 患者中(低、中、高 SSII 分别为 1.8%、9.7%和 10.0%,p=0.004)和在 SSII 较高的 MT 患者中(低、中、高 SSII 分别为 5.0%、4.7%和 10.8%,p=0.031)。与 SS 和 rSS 相比,SSII 对死亡率的预测准确性更好(c 指数=0.62)。
冠状动脉粥样硬化负担本身与全因死亡率显著增加无关。SSII 更好地区分了死亡风险。
ISRCTN66068876。