Division of Hepatobiliary Surgery, The First Affiliated Hospital of Guangxi Medical University, Nanning, 530021, Guangxi, China.
Key Laboratory of Early Prevention and Treatment for Regional High Frequency Tumor (Guangxi Medical University), Ministry of Education, Nanning, 530021, Guangxi, China.
BMC Surg. 2022 Sep 22;22(1):348. doi: 10.1186/s12893-022-01797-4.
There is no general consensus on the feasibility and safety of robotic pancreatoduodenectomy (RPD) and whether it increases surgical risks. The purpose of this study was to assess the safety, feasibility, and rationality of RPD by comparing perioperative data among open pancreatoduodenectomy (OPD), laparoscopic pancreatoduodenectomy (LPD), and RPD performed in our center in recent years.
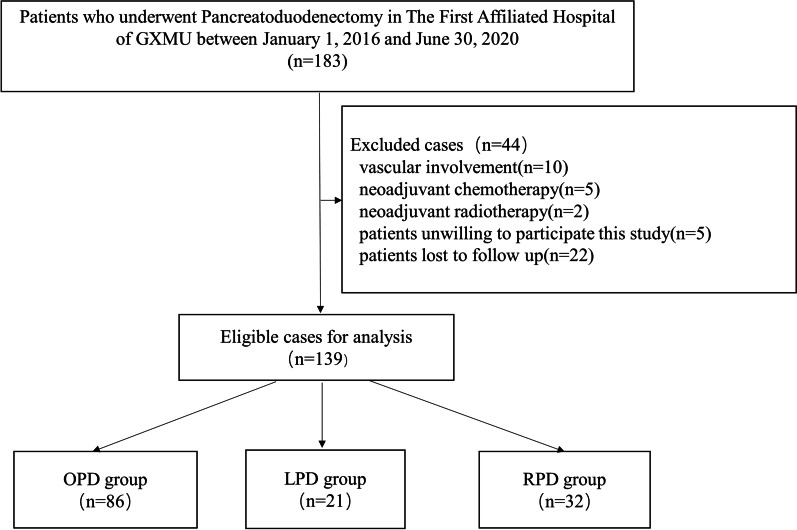
Clinical data of patients had undergone RPD (n = 32), LPD (n = 21), and OPD (n = 86) in The First Affiliated Hospital of Guangxi Medical University between January 2016 and June 2020 were retrospectively collected and analyzed.
RPD required more time for operation (537.2 min vs. 441.5 min, p < 0.001) than OPD did, but less time to remove abdominal drainage tube (12.5 d vs. 17.3 d, p = 0.001). The differences between the RPD group and LPD group were interesting, as the two groups had similar operation time (537.2 min vs. 592.9 min, p = 1.000) and blood loss (482.8 ml vs. 559.5 ml, p > 0.05), but the RPD group had a higher activity of daily living score on postoperative day 3 (35.8 vs. 25.7, p = 0.0017) and a lower rate of conversion to OPD (6.5% vs. 38.1%, p = 0.011). Regarding complications, such as the postoperative pancreatic fistula, abdominal hemorrhage, intra-abdominal infection, bile leakage, reoperation, and perioperative mortality, there were no significant differences among the three groups.
Not only is RPD feasible and reliable, it also offers significant advantages in that it improves postoperative recovery of skills needed for everyday life, has a low conversion rate to open surgery, and does not increase surgical risks.
机器人胰十二指肠切除术(RPD)的可行性和安全性尚无共识,也不确定其是否会增加手术风险。本研究旨在通过比较我院近年来行开放胰十二指肠切除术(OPD)、腹腔镜胰十二指肠切除术(LPD)和 RPD 的围手术期数据来评估 RPD 的安全性、可行性和合理性。
回顾性收集 2016 年 1 月至 2020 年 6 月在广西医科大学第一附属医院行 RPD(n=32)、LPD(n=21)和 OPD(n=86)的患者临床资料,并进行分析。
RPD 的手术时间(537.2 分钟比 441.5 分钟,p<0.001)长于 OPD,但拔除腹腔引流管的时间(12.5 天比 17.3 天,p=0.001)短。RPD 组与 LPD 组的差异很有趣,两组的手术时间(537.2 分钟比 592.9 分钟,p=1.000)和出血量(482.8 毫升比 559.5 毫升,p>0.05)相似,但 RPD 组术后第 3 天的日常生活活动评分更高(35.8 比 25.7,p=0.0017),中转 OPD 的比例更低(6.5%比 38.1%,p=0.011)。术后胰瘘、腹腔出血、腹腔感染、胆漏、再次手术和围手术期死亡率等并发症方面三组之间无显著差异。
RPD 不仅可行可靠,还具有显著优势,可改善术后日常生活所需技能的恢复,中转开腹率低,且不增加手术风险。