Mahidol Oxford Tropical Medicine Research Unit, Faculty of Tropical Medicine, Mahidol University, Bangkok, Thailand; Centre for Tropical Medicine and Global Health, Nuffield Department of Clinical Medicine, University of Oxford, Oxford, UK.
National Center for Parasitology, Entomology and Malaria Control, Phnom Penh, Cambodia.
Lancet Infect Dis. 2023 Jan;23(1):81-90. doi: 10.1016/S1473-3099(22)00492-3. Epub 2022 Sep 26.
Malaria in the eastern Greater Mekong subregion has declined to historic lows. Countries in the Greater Mekong subregion are accelerating malaria elimination in the context of increasing antimalarial drug resistance. Infections are now increasingly concentrated in remote, forested foci. No intervention has yet shown satisfactory efficacy against forest-acquired malaria. The aim of this study was to assess the efficacy of malaria chemoprophylaxis among forest goers in Cambodia.
We conducted an open-label, individually randomised controlled trial in Cambodia, which recruited participants aged 16-65 years staying overnight in forests. Participants were randomly allocated 1:1 to antimalarial chemoprophylaxis, a 3-day course of twice-daily artemether-lumefantrine followed by the same daily dosing once a week while travelling in the forest and for a further 4 weeks after leaving the forest (four tablets per dose; 20 mg of artemether and 120 mg of lumefantrine per tablet), or a multivitamin with no antimalarial activity. Allocations were done according to a computer-generated randomisation schedule, and randomisation was in permuted blocks of size ten and stratified by village. Investigators and participants were not masked to drug allocation, but laboratory investigations were done without knowledge of allocation. The primary outcome was a composite endpoint of either clinical malaria with any Plasmodium species within 1-28, 29-56, or 57-84 days, or subclinical infection detected by PCR on days 28, 56, or 84 using complete-case analysis of the intention-to-treat population. Adherence to study drug was assessed primarily by self-reporting during follow-up visits. Adverse events were assessed in the intention-to-treat population as a secondary endpoint from self-reporting at any time, plus a physical examination and symptom questionnaire at follow-up. This trial is registered at ClinicalTrials.gov (NCT04041973) and is complete.
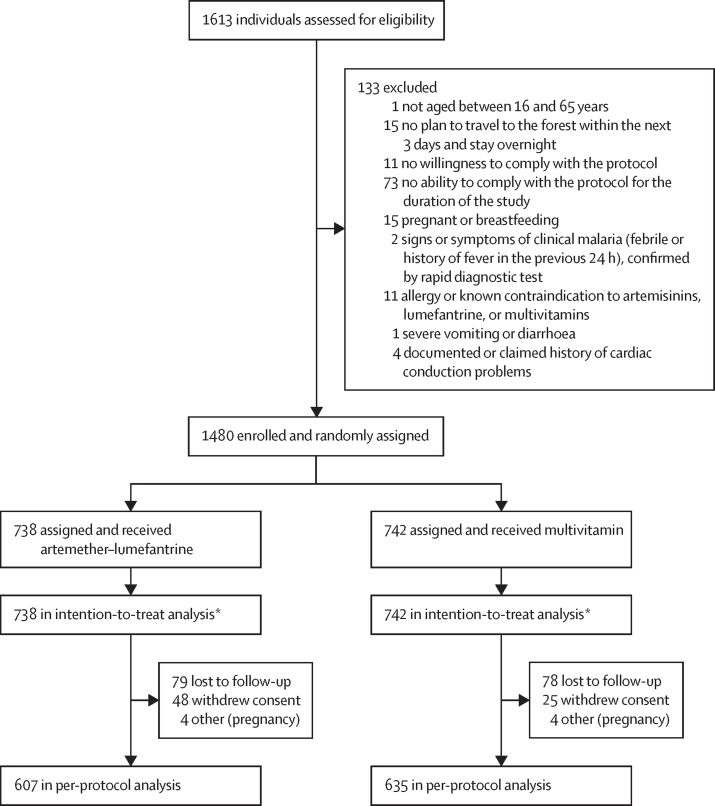
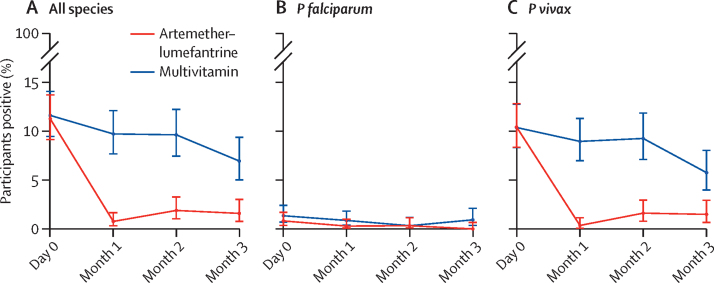
Between March 11 and Nov 20, 2020, 1480 individuals were enrolled, of whom 738 were randomly assigned to artemether-lumefantrine and 742 to the multivitamin. 713 participants in the artemether-lumefantrine group and 714 in the multivitamin group had a PCR result or confirmed clinical malaria by rapid diagnostic test during follow-up. During follow-up, 19 (3%, 95% CI 2-4) of 713 participants had parasitaemia or clinical malaria in the artemether-lumefantrine group and 123 (17%, 15-20) of 714 in the multivitamin group (absolute risk difference 15%, 95% CI 12-18; p<0·0001). During follow-up, there were 166 malaria episodes caused by Plasmodium vivax, 14 by Plasmodium falciparum, and five with other or mixed species infections. The numbers of participants with P vivax were 18 (3%, 95% CI 2-4) in the artemether-lumefantrine group versus 112 (16%, 13-19) in the multivitamin group (absolute risk difference 13%, 95% CI 10-16; p<0·0001). The numbers of participants with P falciparum were two (0·3%, 95% CI 0·03-1·01) in the artemether-lumefantrine group versus 12 (1·7%, 0·9-2·9) in the multivitamin group (absolute risk difference 1·4%, 95% CI 0·4-2·4; p=0·013). Overall reported adherence to the full course of medication was 97% (95% CI 96-98; 1797 completed courses out of 1854 courses started) in the artemether-lumefantrine group and 98% (97-98; 1842 completed courses in 1885 courses started) in the multivitamin group. Overall prevalence of adverse events was 1·9% (355 events in 18 806 doses) in the artemether-lumefantrine group and 1·1% (207 events in 19 132 doses) in the multivitamin group (p<0·0001).
Antimalarial chemoprophylaxis with artemether-lumefantrine was acceptable and well tolerated and substantially reduced the risk of malaria. Malaria chemoprophylaxis among high-risk groups such as forest workers could be a valuable tool for accelerating elimination in the Greater Mekong subregion.
The Global Fund to Fight AIDS, Tuberculosis and Malaria; Wellcome Trust.
大湄公河次区域东部的疟疾已降至历史新低。在抗疟药物耐药性不断增加的情况下,大湄公河次区域国家正在加速消除疟疾。目前感染病例越来越集中在偏远的森林地区。迄今尚无干预措施对森林获得性疟疾显示出令人满意的疗效。本研究旨在评估柬埔寨森林工作者中疟疾化学预防的效果。
我们在柬埔寨进行了一项开放标签、个体随机对照试验,招募了在森林中过夜的 16-65 岁的参与者。参与者被随机分配 1:1 接受抗疟化学预防,即服用 3 天的双日剂量青蒿琥酯-咯萘啶,然后在森林中旅行时每周服用相同剂量,持续 4 周,离开森林后再服用 4 周(每次剂量 4 片;每片含青蒿琥酯 20 毫克和咯萘啶 120 毫克),或服用不含抗疟活性的多种维生素。所有分配均根据计算机生成的随机分配方案进行,随机分配按大小为 10 的置换块和村庄分层进行。调查人员和参与者均未对药物分配进行盲法,但实验室检查是在不知道分配的情况下进行的。主要结局是复合终点,即在 1-28、29-56 或 57-84 天内任何一种疟原虫物种引起的临床疟疾,或在第 28、56 或 84 天通过 PCR 检测到亚临床感染,采用意向治疗人群的完整病例分析。通过随访时的自我报告主要评估对研究药物的依从性。不良事件作为次要终点,在任何时间进行自我报告,并在随访时进行体格检查和症状问卷评估,均在意向治疗人群中进行评估。本试验在 ClinicalTrials.gov(NCT04041973)注册,现已完成。
在 2020 年 3 月 11 日至 11 月 20 日期间,共纳入了 1480 名参与者,其中 738 名被随机分配至青蒿琥酯-咯萘啶组,742 名被分配至多种维生素组。在随访期间,713 名青蒿琥酯-咯萘啶组和 714 名多种维生素组的参与者中,有 713 名有 PCR 结果或快速诊断试验证实的临床疟疾。在随访期间,青蒿琥酯-咯萘啶组中有 19 例(3%,95%CI 2-4)发生寄生虫血症或临床疟疾,而多种维生素组中有 123 例(17%,15-20)发生寄生虫血症或临床疟疾(绝对风险差异 15%,95%CI 12-18;p<0·0001)。在随访期间,共有 166 例疟疾病例由间日疟原虫引起,14 例由恶性疟原虫引起,5 例由其他或混合物种感染引起。间日疟原虫的参与者人数为青蒿琥酯-咯萘啶组 18 例(3%,95%CI 2-4),多种维生素组 112 例(16%,13-19)(绝对风险差异 13%,95%CI 10-16;p<0·0001)。恶性疟原虫的参与者人数为青蒿琥酯-咯萘啶组 2 例(0·3%,95%CI 0·03-1·01),多种维生素组 12 例(1·7%,0·9-2·9)(绝对风险差异 1·4%,95%CI 0·4-2·4;p=0·013)。在青蒿琥酯-咯萘啶组中,1854 个疗程中有 1797 个完成(97%,95%CI 96-98),在多种维生素组中,1885 个疗程中有 1842 个完成(98%,97-98),报告的总体药物依从性良好。在青蒿琥酯-咯萘啶组中,不良事件的总发生率为 1·9%(1806 剂 355 例),在多种维生素组中为 1·1%(19132 剂 207 例)(p<0·0001)。
青蒿琥酯-咯萘啶抗疟化学预防是可以接受的,且耐受性良好,大大降低了疟疾的风险。对于森林工人等高危人群,疟疾化学预防可能是加速大湄公河次区域消除疟疾的一项宝贵工具。
全球抗击艾滋病、结核病和疟疾基金;惠康信托基金会。