Department of Medicine (Gastroenterology and Hepatology) and Department of Epidemiology and Population Health, Stanford University Medical Center, Palo Alto, California, USA.
Mayo Clinic, Rochester, Minnesota, USA.
Hepatol Commun. 2022 Dec;6(12):3443-3456. doi: 10.1002/hep4.2087. Epub 2022 Sep 30.
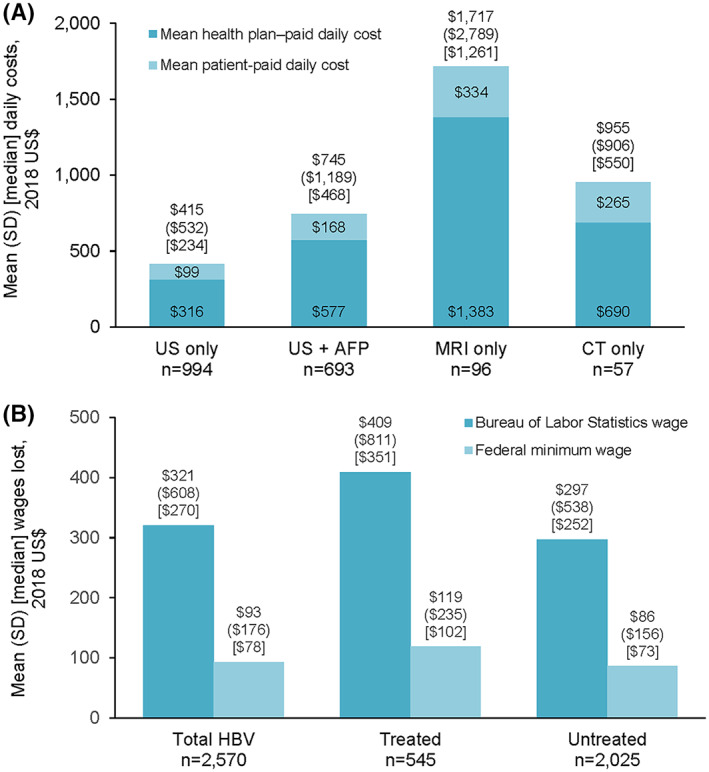
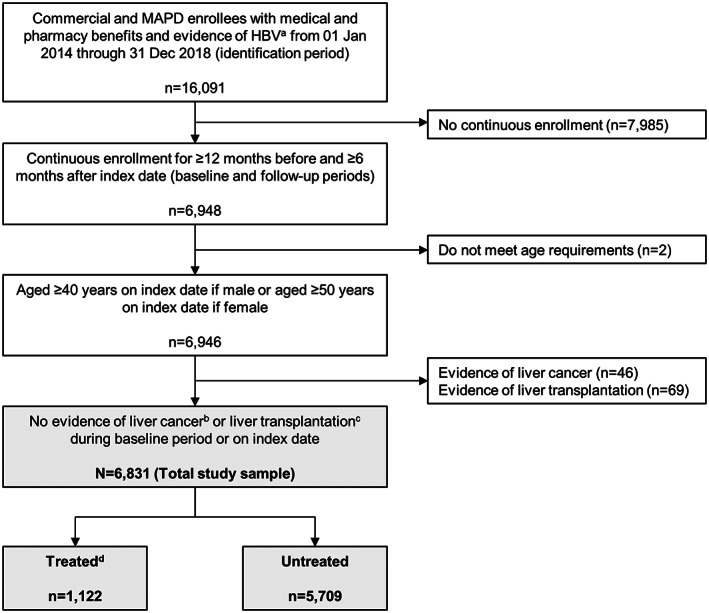
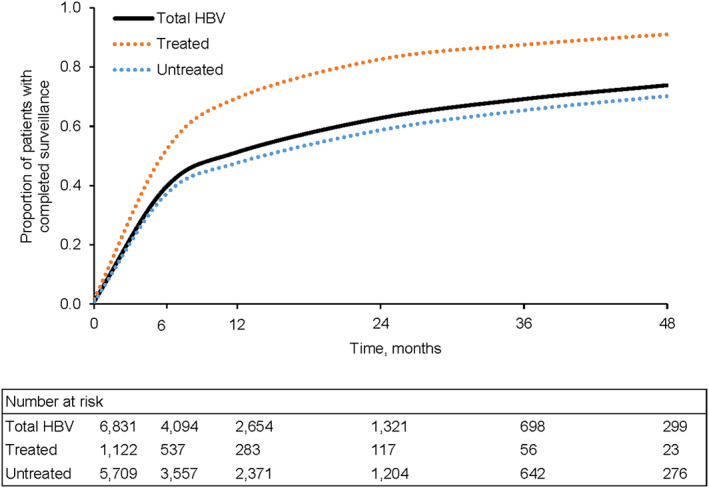
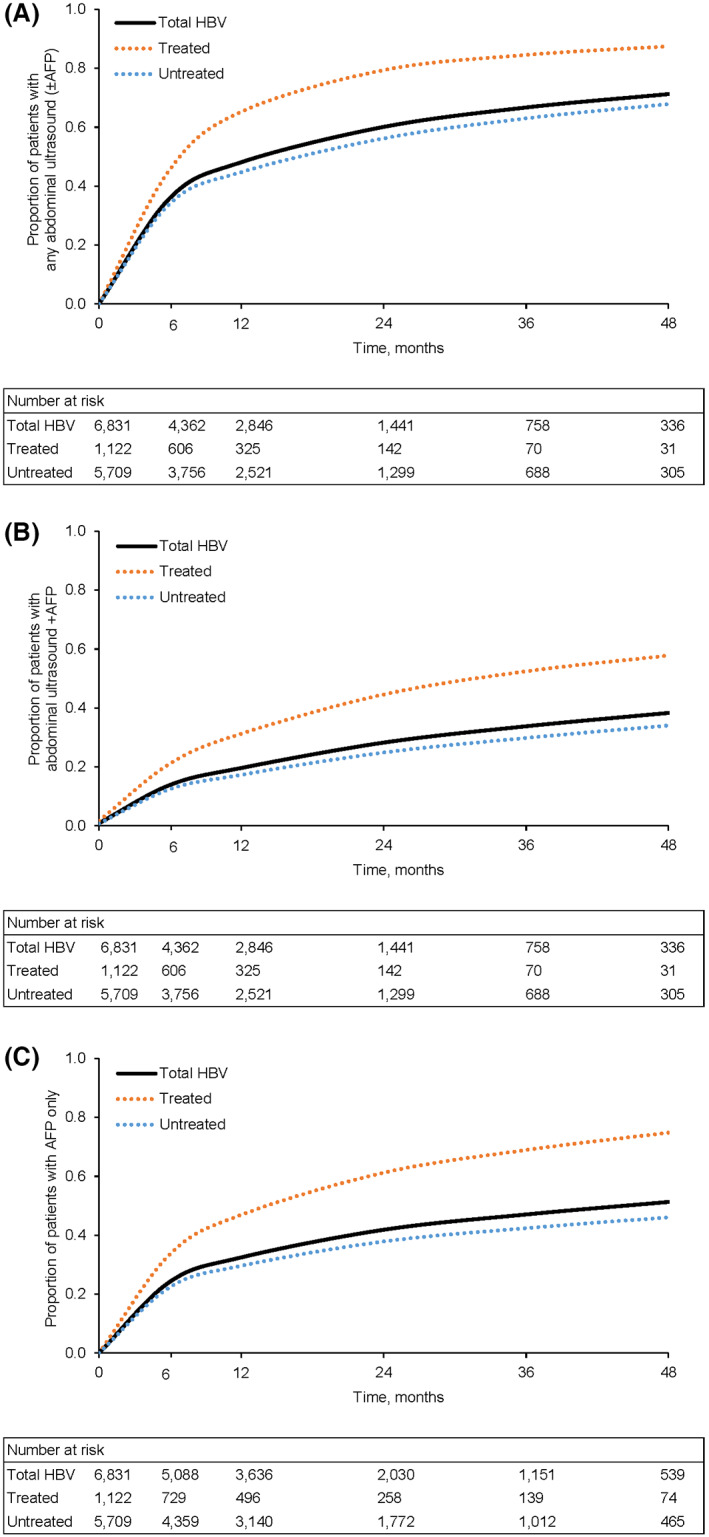
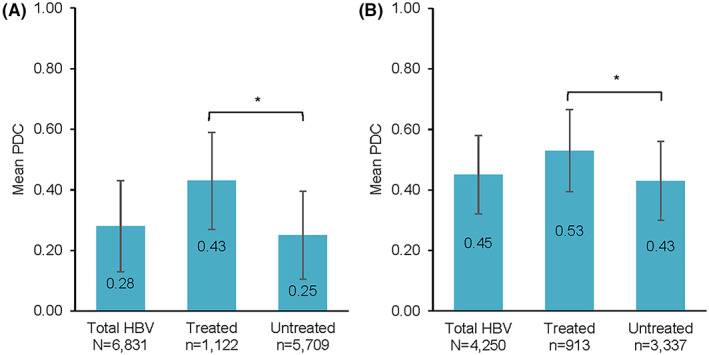
Suboptimal adherence to guidelines for hepatocellular carcinoma (HCC) surveillance among high-risk patients is a persistent problem with substantial detriment to patient outcomes. While patients cite cost as a barrier to surveillance receipt, the financial burden they experience due to surveillance has not been examined. We conducted a retrospective administrative claims study to assess HCC surveillance use and associated costs in a US cohort of insured patients without cirrhosis but with hepatitis B virus (HBV) infection, monitored in routine clinical practice. Of 6831 patients (1122 on antiviral treatment, 5709 untreated), only 39.3% and 51.3% had received any abdominal imaging after 6 and 12 months, respectively, and patients were up to date with HCC surveillance guidelines for only 28% of the follow-up time. Completion of surveillance was substantially higher at 6 and 12 months among treated patients (51.7% and 69.6%, respectively) compared with untreated patients (36.9% and 47.6%, respectively) (p < 0.001). In adjusted models, treated patients were more likely than untreated patients to receive surveillance (hazard ratio [HR] 1.75, 95% confidence interval [CI] 1.53-2.01, p < 0.001), and the proportion of those up to date with surveillance was 9.7% higher (95% CI 6.26-13.07, p < 0.001). Mean total and patient-paid daily surveillance-related costs ranged from $99 (ultrasound) to $334 (magnetic resonance imaging), and mean annual patient costs due to lost productivity for surveillance-related outpatient visits ranged from $93 (using the federal minimum wage) to $321 (using the Bureau of Labor Statistics wage). Conclusion: Use of current HCC surveillance strategies was low across patients with HBV infection, and surveillance was associated with substantial patient financial burden. These data highlight an urgent need for accessible and easy-to-implement surveillance strategies with sufficient sensitivity and specificity for early HCC detection.
高危患者对肝细胞癌 (HCC) 监测指南的依从性不理想是一个持续存在的问题,对患者的预后有实质性的影响。虽然患者认为成本是接受监测的障碍,但他们因监测而经历的经济负担尚未得到检查。我们进行了一项回顾性行政索赔研究,以评估在美国没有肝硬化但患有乙型肝炎病毒 (HBV) 感染的参保患者队列中,在常规临床实践中监测 HCC 监测的使用情况和相关费用。在 6831 名患者中(1122 名接受抗病毒治疗,5709 名未接受治疗),只有 39.3%和 51.3%在 6 个月和 12 个月后分别接受了任何腹部影像学检查,而只有 28%的患者在随访期间符合 HCC 监测指南。与未接受治疗的患者相比,接受治疗的患者在 6 个月和 12 个月时完成监测的比例明显更高(分别为 51.7%和 69.6%)(p<0.001)。在调整后的模型中,与未接受治疗的患者相比,接受治疗的患者更有可能接受监测(风险比 [HR] 1.75,95%置信区间 [CI] 1.53-2.01,p<0.001),并且符合监测要求的比例高 9.7%(95% CI 6.26-13.07,p<0.001)。总和患者自付的每日与监测相关的费用范围从 99 美元(超声)到 334 美元(磁共振成像)不等,由于与监测相关的门诊就诊而导致的患者每年生产力损失的费用范围从 93 美元(使用联邦最低工资)到 321 美元(使用劳工统计局工资)不等。结论:在 HBV 感染患者中,当前 HCC 监测策略的使用率较低,并且监测与患者的巨大经济负担有关。这些数据突出表明,迫切需要具有足够敏感性和特异性的易于获得和易于实施的监测策略,以早期发现 HCC。