Cardiovascular Division, Brigham and Women's Hospital, Harvard Medical School, Boston, MA, USA.
Minneapolis VA Center for Care Delivery and Outcomes Research, University of Minnesota, Minneapolis, MN, USA.
Eur J Heart Fail. 2023 Jan;25(1):87-94. doi: 10.1002/ejhf.2703. Epub 2022 Oct 27.
As sacubitril/valsartan may potentiate early natriuresis, expert consensus documents recommend diuretic dose reduction on first initiation. However, there are limited data on the effects of sacubitril/valsartan on the background of varying diuretic regimens or on diuretic requirements over time in heart failure (HF) with preserved ejection fraction (HFpEF).
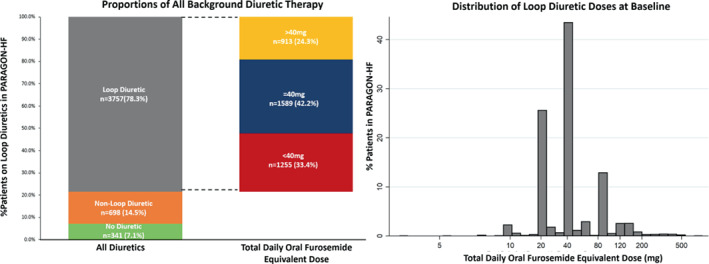
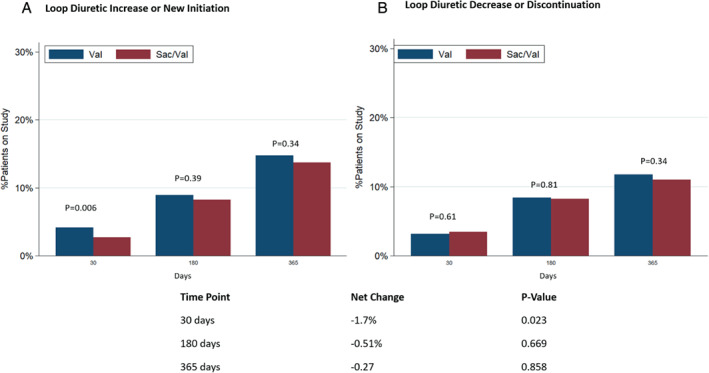
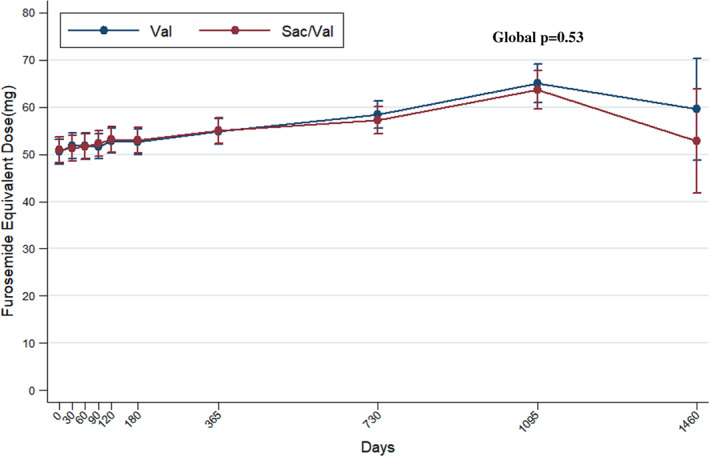
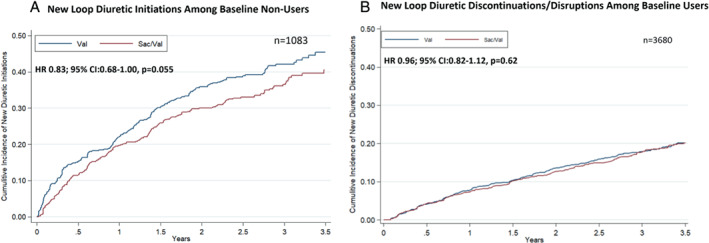
In this post hoc analysis of PARAGON-HF, of the 4796 patients, background diuretic therapy was distributed as follows: 341 (7%) on no diuretic, 698 (15%) on non-loop diuretic, and 3757 (78%) were on loop diuretics (1255, 1589, and 913 were on <40, 40 and >40 mg furosemide equivalent doses, respectively). The primary composite outcome of total HF hospitalizations and cardiovascular death was analysed using semiparametric proportional rates methods. The cumulative incidence of the primary composite outcome (first events) was lowest in patients on no diuretic and highest in those on >40 mg of loop diuretic (p < 0.001). The effects of sacubitril/valsartan (vs. valsartan) on the primary composite outcome (recurrent events) did not significantly vary by baseline diuretic use (p = 0.65). Treatment effects on safety outcomes were similar across diuretic categories. Sacubitril/valsartan reduced new loop diuretic initiations over the course of the trial (hazard ratio 0.83; 95% confidence interval 0.68-1.00, p = 0.055), with similar mean loop diuretic dose and rates of diuretic discontinuation between treatment groups in follow-up. Patients randomized to sacubitril/valsartan experienced a slight early reduction in diuretic initiation or dose escalation at 30 days after initiation (net reduction 1.7%, p = 0.02), but these differences were not sustained beyond this timepoint.
Patients with HFpEF on higher baseline diuretic doses were at heightened risk of HF events, but similarly benefited from sacubitril/valsartan with a consistent safety profile across a range of diuretic doses. Initiation of sacubitril/valsartan was associated with modestly lower new loop diuretic requirement in follow-up.
由于沙库巴曲缬沙坦可能增强早期利钠作用,专家共识文件建议在首次使用时减少利尿剂剂量。然而,在射血分数保留的心力衰竭(HFpEF)中,关于沙库巴曲缬沙坦对不同利尿剂方案背景或随时间推移的利尿剂需求的影响的数据有限。
在 PARAGON-HF 的这项事后分析中,4796 例患者中,背景利尿剂治疗分布如下:341 例(7%)无利尿剂,698 例(15%)非袢利尿剂,3757 例(78%)为袢利尿剂(1255、1589 和 913 例分别为<40、40 和>40mg 呋塞米等效剂量)。使用半参数比例风险方法分析主要复合终点(全因 HF 住院和心血管死亡)。无利尿剂患者的主要复合终点(首发事件)累积发生率最低,而>40mg 袢利尿剂患者的累积发生率最高(p<0.001)。沙库巴曲缬沙坦(与缬沙坦相比)对主要复合终点(复发性事件)的影响在基线利尿剂使用方面无显著差异(p=0.65)。在利尿剂类别中,治疗效果对安全性结局的影响相似。沙库巴曲缬沙坦在试验过程中减少了新的袢利尿剂的起始使用(风险比 0.83;95%置信区间 0.68-1.00,p=0.055),在随访中,治疗组之间的平均袢利尿剂剂量和利尿剂停药率相似。与接受缬沙坦治疗的患者相比,接受沙库巴曲缬沙坦治疗的患者在起始后 30 天内利尿剂起始或剂量升级的情况略有早期减少(净减少 1.7%,p=0.02),但这些差异在此时点后并未持续。
基线利尿剂剂量较高的 HFpEF 患者发生 HF 事件的风险较高,但同样受益于沙库巴曲缬沙坦,且在一系列利尿剂剂量下具有一致的安全性。沙库巴曲缬沙坦的起始使用与随访中新型袢利尿剂需求适度降低相关。