Ezeigwe Angelica, Ogunmoroti Oluseye, Minhas Anum S, Rodriguez Carla P, Kazzi Brigitte, Fashanu Oluwaseun E, Osibogun Olatokunbo, Kovell Lara C, Harrington Colleen M, Michos Erin D
Ciccarone Center for the Prevention of Cardiovascular Disease, Johns Hopkins University School of Medicine, Baltimore, MD, United States.
Division of Cardiology, Sands Constellation Heart Institute, Rochester Regional Health, Rochester, NY, United States.
Front Cardiovasc Med. 2022 Sep 14;9:922367. doi: 10.3389/fcvm.2022.922367. eCollection 2022.
Multiparity has been associated with increased risk of cardiovascular disease (CVD). Inflammation may be a mechanism linking parity to CVD. We investigated the association between parity and later-life markers of inflammation.
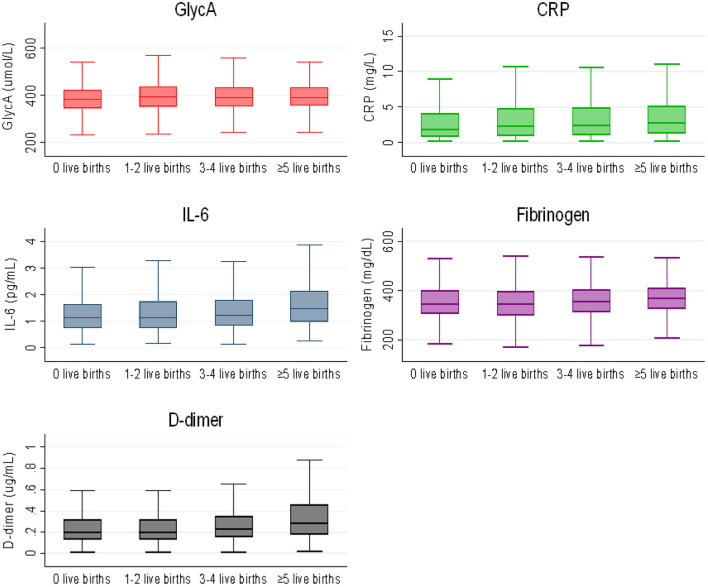
We studied 3,454 female MESA participants aged 45-84, free of CVD, who had data on parity and inflammatory markers. Parity was categorized as 0 (reference), 1-2, 3-4, or ≥5. Linear regression was used to evaluate the association between parity and natural log-transformed levels of fibrinogen, D-dimer, GlycA, high sensitivity C-reactive protein (hsCRP), and interleukin-6 (IL-6).
Mean age was 62 ± 10 years. The proportion of women with nulliparity, 1-2, 3-4, and ≥5 live births were 18, 39, 29, and 14%, respectively. There was no association between parity and fibrinogen. Women with grand multiparity (≥5 live births) had 28, 10, and 18% higher levels of hsCRP, IL-6 and D-dimer, respectively, compared to nulliparous women, after adjustment for demographic factors. After additional adjustment for CVD risk factors, women with 1-2 and 3-4 live births had higher hsCRP and women with 1-2 live births had higher GlycA.
In this diverse cohort of middle-to-older aged women, we found that higher parity was associated with some inflammatory markers; however, these associations were largely attenuated after adjustment for CVD risk factors. There was no clear dose-response relationship between parity and these inflammatory markers. Future studies are needed to evaluate how inflammation may influence the link between parity and CVD and whether healthy lifestyle/pharmacotherapies targeting inflammation can reduce CVD risk among multiparous women.
The MESA cohort design is registered at clinicaltrials.gov as follows: https://clinicaltrials.gov/ct2/show/NCT00005487.
多产与心血管疾病(CVD)风险增加有关。炎症可能是连接生育与心血管疾病的一种机制。我们研究了生育与晚年炎症标志物之间的关联。
我们研究了3454名年龄在45 - 84岁、无心血管疾病的女性MESA参与者,她们有生育情况和炎症标志物的数据。生育情况分为0(参照组)、1 - 2次、3 - 4次或≥5次。采用线性回归来评估生育情况与纤维蛋白原、D - 二聚体、糖化白蛋白(GlycA)、高敏C反应蛋白(hsCRP)和白细胞介素 - 6(IL - 6)自然对数转换水平之间的关联。
平均年龄为62±10岁。未生育、生育1 - 2次、生育3 - 4次和生育≥5次妇女的比例分别为18%、39%、29%和14%。生育情况与纤维蛋白原之间无关联。在调整人口统计学因素后,多产(生育≥5次)妇女的hsCRP水平、IL - 6水平和D - 二聚体水平分别比未生育妇女高28%、10%和18%。在进一步调整心血管疾病危险因素后,生育1 - 2次和生育3 - 4次的妇女hsCRP水平较高,生育1 - 2次的妇女GlycA水平较高。
在这个年龄跨度从中年到老年的不同队列女性中,我们发现较高的生育次数与一些炎症标志物有关;然而,在调整心血管疾病危险因素后,这些关联大多减弱。生育次数与这些炎症标志物之间没有明确的剂量反应关系。未来需要开展研究,以评估炎症如何影响生育与心血管疾病之间的联系,以及针对炎症的健康生活方式/药物治疗是否能降低多产妇女的心血管疾病风险。
MESA队列设计在clinicaltrials.gov上的注册信息如下:https://clinicaltrials.gov/ct2/show/NCT00005487 。