Agarwal Ankita, Chen Jen-Ting, Coopersmith Craig M, Denson Joshua L, Dickert Neal W, Ferrante Lauren E, Gershengorn Hayley B, Gosine Adhiraj D, Hayward Bradley J, Kaur Navneet, Khan Akram, Lamberton Courtney, Landsittel Douglas, Lyons Patrick G, Mikkelsen Mark E, Nadig Nandita R, Pietropaoli Anthony P, Poole Brian R, Viglianti Elizabeth M, Sevransky Jonathan E
Division of Pulmonary, Allergy, Critical Care and Sleep Medicine, Department of Medicine, Emory University School of Medicine, Atlanta, GA.
Emory Critical Care Center, Emory Healthcare, Atlanta, GA.
Crit Care Explor. 2022 Oct 13;4(10):e0774. doi: 10.1097/CCE.0000000000000774. eCollection 2022 Oct.
The optimal staffing model for physicians in the ICU is unknown. Patient-to-intensivist ratios may offer a simple measure of workload and be associated with patient mortality and physician burnout. To evaluate the association of physician workload, as measured by the patient-to-intensivist ratio, with physician burnout and patient mortality.
Cross-sectional observational study.
Fourteen academic centers in the United States from August 2020 to July 2021.
We enrolled ICU physicians and collected data on adult ICU patients under the physician's care on the single physician-selected study day for each physician.
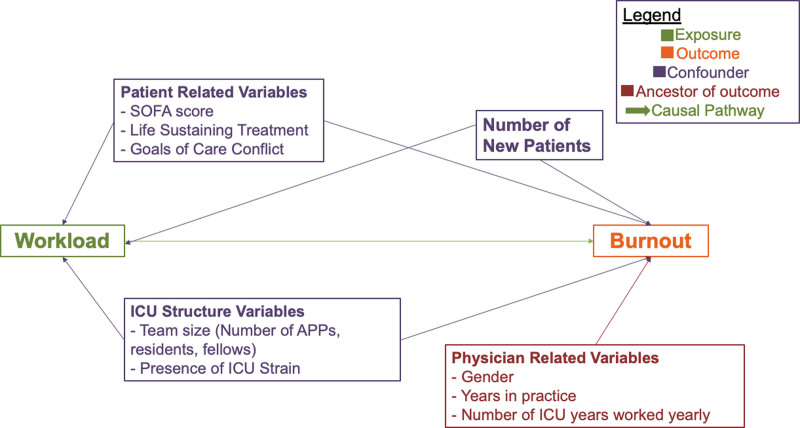
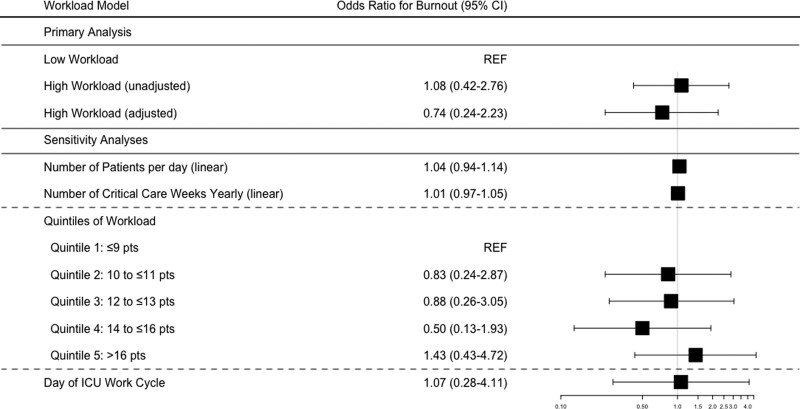
The primary exposure was workload (self-reported number of patients' physician was responsible for) modeled as high (>14 patients) and low (≤14 patients). The primary outcome was burnout, measured by the Well-Being Index. The secondary outcome measure was 28-day patient mortality. We calculated odds ratio for burnout and patient outcomes using a multivariable logistic regression model and a binomial mixed effects model, respectively. We enrolled 122 physicians from 62 ICUs. The median patient-to-intensivist ratio was 12 (interquartile range, 10-14), and the overall prevalence of burnout was 26.4% ( = 32). Intensivist workload was not independently associated with burnout (adjusted odds ratio, 0.74; 95% CI, 0.24-2.23). Of 1,322 patients, 679 (52%) were discharged alive from the hospital, 257 (19%) remained hospitalized, and 347 (26%) were deceased by day 28; 28-day outcomes were unknown for 39 of patients (3%). Intensivist workload was not independently associated with 28-day patient mortality (adjusted odds ratio, 1.33; 95% CI, 0.92-1.91).
In our cohort, approximately one in four physicians experienced burnout on the study day. There was no relationship be- tween workload as measured by patient-to-intensivist ratio and burnout. Factors other than the number of patients may be important drivers of burnout among ICU physicians.
重症监护病房(ICU)中医生的最佳人员配置模式尚不清楚。患者与重症监护医生的比例可能提供一种简单的工作量衡量指标,并与患者死亡率和医生职业倦怠相关。评估以患者与重症监护医生的比例衡量的医生工作量与医生职业倦怠和患者死亡率之间的关联。
横断面观察性研究。
2020年8月至2021年7月期间美国的14个学术中心。
我们招募了ICU医生,并收集了每位医生在其自行选择的研究日负责护理的成年ICU患者的数据。
主要暴露因素是工作量(医生自我报告负责的患者数量),分为高(>14名患者)和低(≤14名患者)两种情况。主要结局是职业倦怠,通过幸福感指数来衡量。次要结局指标是28天患者死亡率。我们分别使用多变量逻辑回归模型和二项混合效应模型计算职业倦怠和患者结局的比值比。我们从62个ICU招募了122名医生。患者与重症监护医生的比例中位数为12(四分位间距,10 - 14),职业倦怠的总体患病率为26.4%(n = 32)。重症监护医生的工作量与职业倦怠无独立相关性(调整后的比值比,0.74;95%置信区间,0.24 - 2.23)。在1322名患者中,679名(52%)出院时存活,257名(19%)仍住院,347名(26%)在第28天时死亡;39名患者(3%)的28天结局未知。重症监护医生的工作量与28天患者死亡率无独立相关性(调整后的比值比,1.33;95%置信区间,0.92 - 1.91)。
在我们的队列中,约四分之一的医生在研究日经历了职业倦怠。以患者与重症监护医生的比例衡量的工作量与职业倦怠之间没有关系。除患者数量外的其他因素可能是ICU医生职业倦怠的重要驱动因素。