Department of Anaesthesiology and Intensive Care Medicine, Medical University of Graz, Auenbruggerplatz 5, 8036, Graz, Austria.
Center for Medical Data Science, Medical University of Vienna, Vienna, Austria.
Crit Care. 2024 Sep 14;28(1):304. doi: 10.1186/s13054-024-05090-z.
Too high or too low patient volumes and work amounts may overwhelm health care professionals and obstruct processes or lead to inadequate personnel routine and process flow. We sought to evaluate, whether an association between current caseload, current workload, and outcomes exists in intensive care units (ICU).
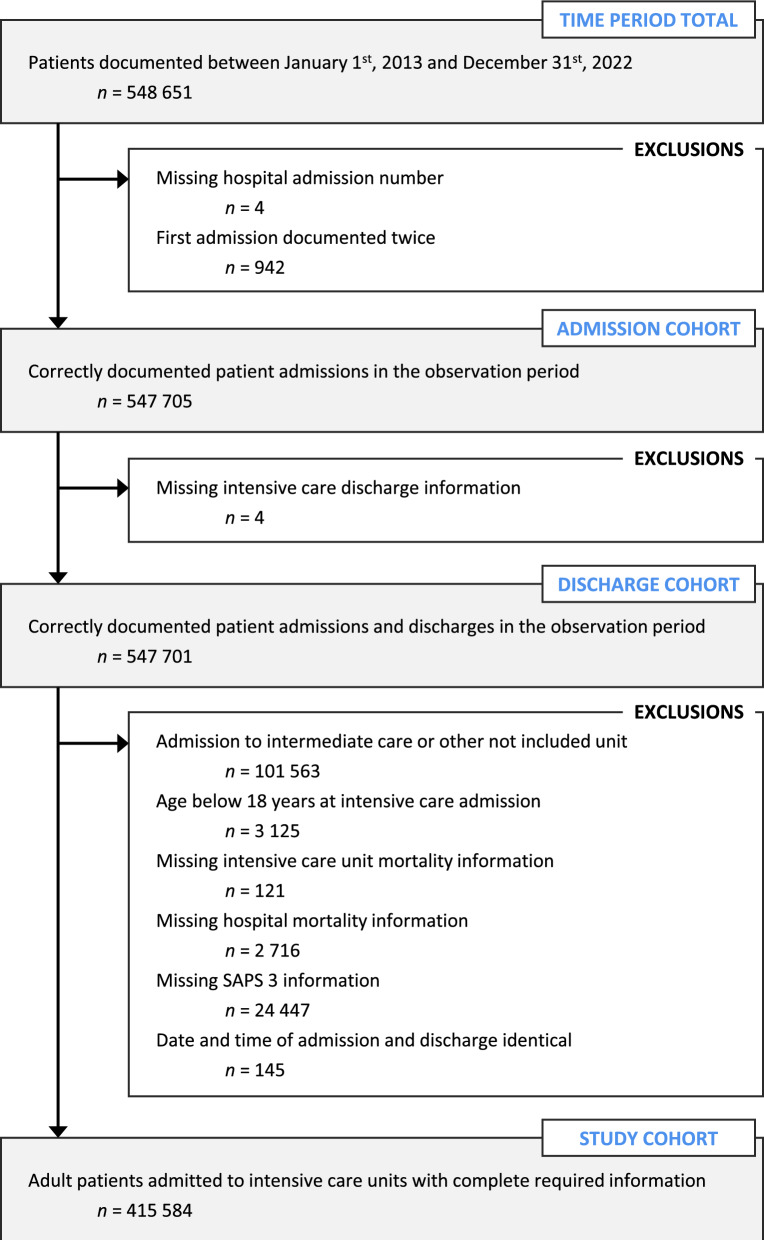
Retrospective cohort analysis of data from an Austrian ICU registry. Data on patients aged ≥ 18 years admitted to 144 Austrian ICUs between 2013 and 2022 were included. A Cox proportional hazards model with ICU mortality as the outcome of interest adjusted with patients' respective SAPS 3, current ICU caseload (measured by ICU occupancy rates), and current ICU workload (measured by median TISS-28 per ICU) as time-dependent covariables was constructed. Subgroup analyses were performed for types of ICUs, hospital care level, and pre-COVID or intra-COVID period.
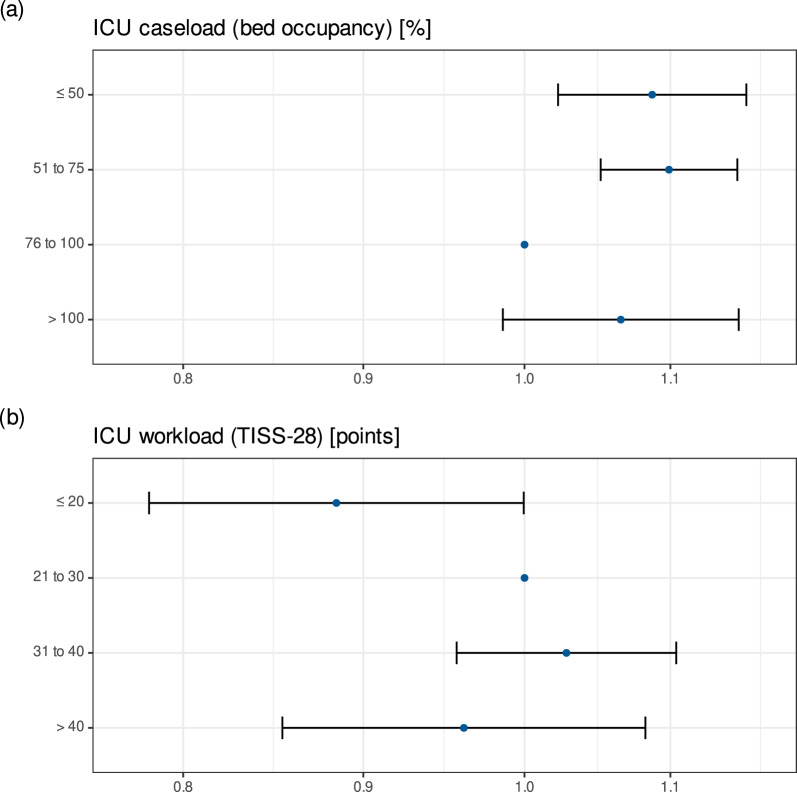
415 584 patient admissions to 144 ICUs were analysed. Compared to ICU caseloads of 76 to 100%, there was no significant relationship between overuse of ICU capacity and risk of death [HR (95% CI) 1.06 (0.99-1.15), p = 0.110 for > 100%], but for lower utilisation [1.09 (1.02-1.16), p = 0.008 for ≤ 50% and 1.10 (1.05-1.15), p < 0.0001 for 51-75%]. Exceptions were significant associations for caseloads > 100% between 2020 and 2022 [1.18 (1.06-1.30), p = 0.001], i.e., the intra-COVID period. Compared to the reference category of median TISS-28 21-30, lower [0.88 (0.78-0.99), p = 0.049 for ≤ 20], but not higher workloads were significantly associated with risk of death. High workload may be associated with higher mortality in local hospitals [1.09 (1.01-1.19), p = 0.035 for 31-40, 1.28 (1.02-1.60), p = 0.033 for > 40].
In a system with comparably high intensive care resources and mandatory staffing levels, patients' survival chances are generally not affected by high intensive care unit caseload and workload. However, extraordinary circumstances, such as the COVID-19 pandemic, may lead to higher risk of death, if planned capacities are exceeded. High workload in ICUs in smaller hospitals with lower staffing levels may be associated with increased risk of death.
过高或过低的患者量和工作量可能会使医疗保健专业人员不堪重负,阻碍流程或导致人员常规和流程不足。我们试图评估当前病例量、当前工作量与重症监护病房(ICU)结局之间是否存在关联。
回顾性队列分析来自奥地利 ICU 登记处的数据。纳入 2013 年至 2022 年间在奥地利 144 家 ICU 住院的年龄≥18 岁的患者。使用 ICU 死亡率作为感兴趣的结局,构建了 Cox 比例风险模型,调整了患者各自的 SAPS 3、当前 ICU 病例量(通过 ICU 入住率衡量)和当前 ICU 工作量(通过中位数 TISS-28 衡量)作为时间依赖性协变量。对 ICU 类型、医院护理水平、COVID-19 前或 COVID-19 期间进行了亚组分析。
分析了来自 144 家 ICU 的 415584 例患者入院数据。与 ICU 容量使用率为 76%至 100%相比,ICU 容量过度使用与死亡风险之间没有显著关系[风险比(HR)(95%置信区间)为 1.06(0.99-1.15),p=0.110],但与使用率较低有关[1.09(1.02-1.16),p=0.008 用于≤50%,1.10(1.05-1.15),p<0.0001 用于 51-75%]。例外情况是 2020 年至 2022 年之间 ICU 病例量超过 100%与死亡率之间存在显著关联[1.18(1.06-1.30),p=0.001],即 COVID-19 期间。与中位数 TISS-28 为 21-30 的参考类别相比,较低的工作量[0.88(0.78-0.99),p=0.049 用于≤20]与死亡风险显著相关,但较高的工作量则没有。高工作量可能与当地医院较高的死亡率有关[1.09(1.01-1.19),p=0.035 用于 31-40,1.28(1.02-1.60),p=0.033 用于>40]。
在一个拥有相对较高的重症监护资源和强制性人员配备水平的系统中,患者的生存机会通常不受高重症监护病房病例量和工作量的影响。然而,在 COVID-19 大流行等特殊情况下,如果计划容量超过,可能会导致更高的死亡风险。人员配备水平较低的小型医院的 ICU 高工作量可能与死亡风险增加有关。