Hwang In-Chang, Choi Hong-Mi, Yoon Yeonyee E, Park Jin Joo, Park Jun-Bean, Park Jae-Hyeong, Lee Seung-Pyo, Kim Hyung-Kwan, Kim Yong-Jin, Cho Goo-Yeong
Department of Cardiology, Cardiovascular Center, Seoul National University Bundang Hospital, Seongnam, Korea.
Department of Internal Medicine, Seoul National University College of Medicine, Seoul, Korea.
Int J Heart Fail. 2022 Apr 4;4(2):95-109. doi: 10.36628/ijhf.2022.0007. eCollection 2022 Apr.
Lower body mass index (BMI) is considered a poor prognostic factor in patients with heart failure (HF). We aimed to investigate the clinical impact of BMI on the risk of mortality in patients with acute HF (AHF) across various phenotypes.
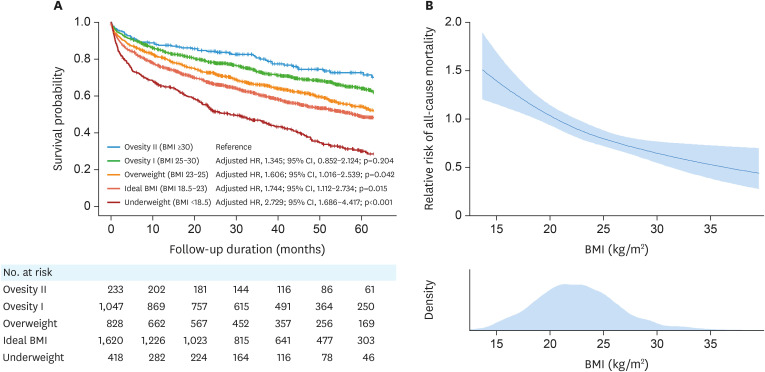
We retrospectively identified 4,146 registry patients with AHF and BMI data. The study population was categorized according to the WHO Asia-Pacific BMI classification: BMI <18.5 kg/m (underweight; n=418), BMI 18.5-23 kg/m (ideal; n=1,620), BMI 23-25 kg/m (overweight; n=828), BMI 25-30 kg/m (obesity I; n=1,047), and BMI ≥30 kg/m (obesity II; n=233). The risk of all-cause mortality was compared between these 5 groups.
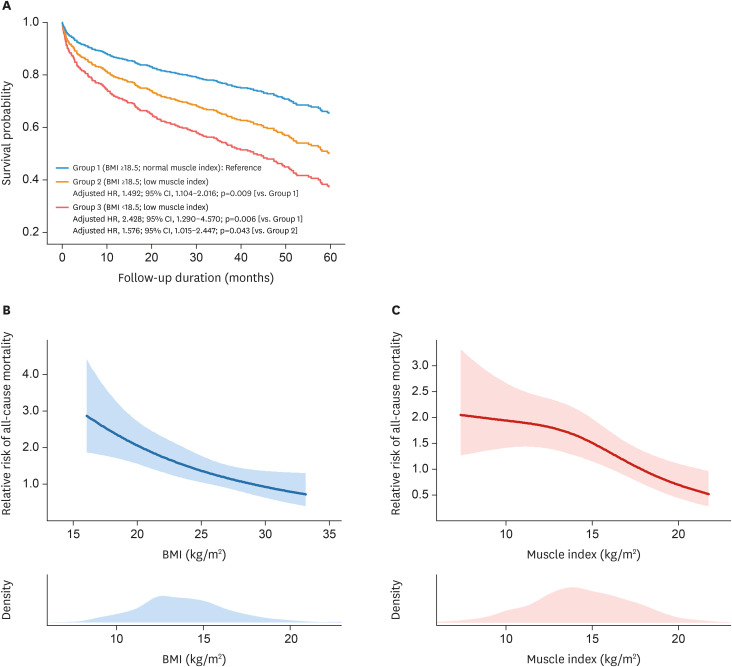
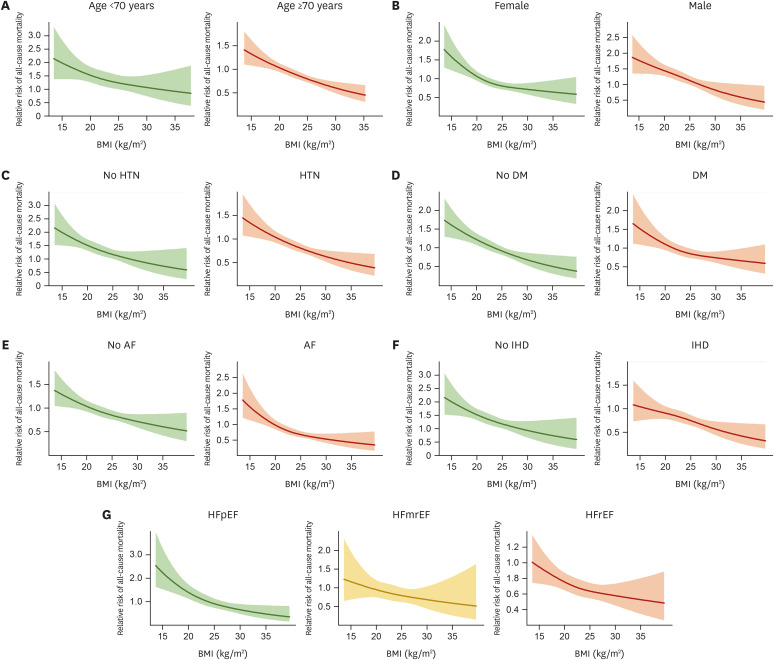
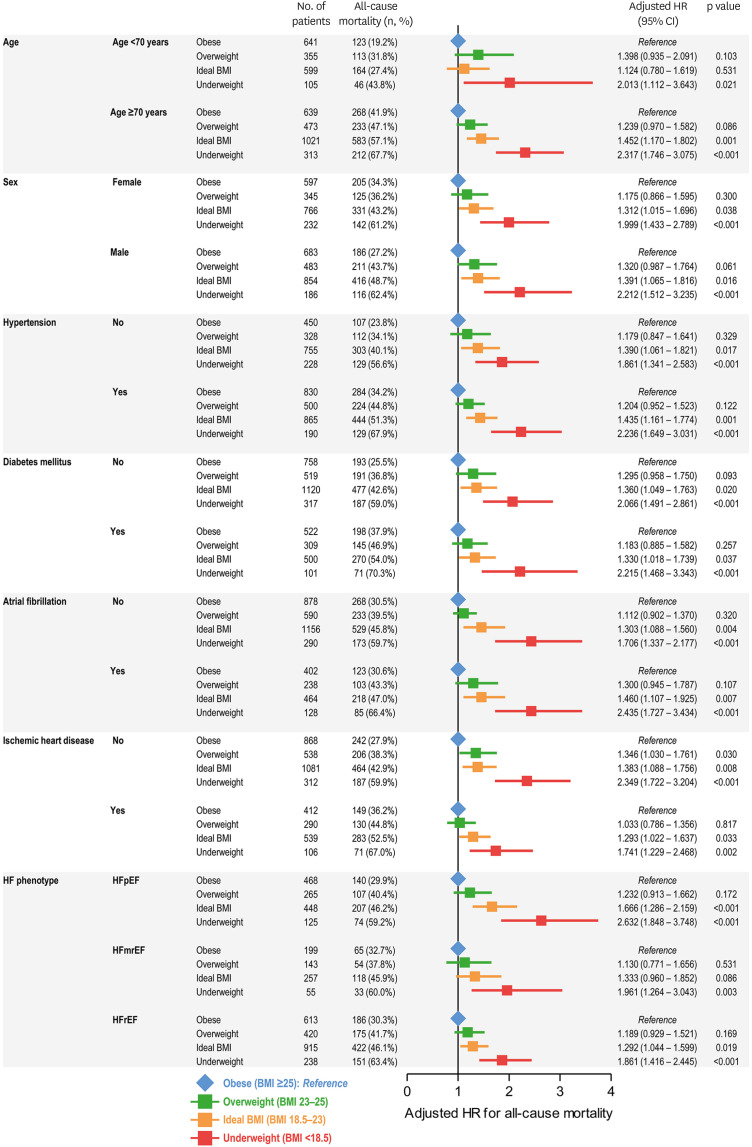
During a median follow-up of 32 months, 1,732 patients (41.8%) died. Compared to patients with obesity II, those with overweight, ideal BMI or underweight status had a higher risk of mortality (overweight: hazard ratio [HR], 1.606; 95% confidence interval [CI], 1.016-2.539; p=0.042) (ideal BMI: HR, 1.744; 95% CI, 1.112-2.734; p=0.015) (underweight: HR, 2.729; 95% CI, 1.686-4.417; p<0.001). Higher risk of mortality among patients with lower BMI was observed regardless of age, sex, hypertension, diabetes, ischemic heart disease, atrial fibrillation, and HF phenotype. Furthermore, low muscle index (total muscle mass/height), calculated using serum cystatin C data in a subset of 579 patients, was associated with higher mortality risk.
A lower BMI is associated with a higher risk of mortality in patients with AHF. This obesity paradox is observed in AHF regardless of comorbidities and HF phenotype.
较低的体重指数(BMI)被认为是心力衰竭(HF)患者预后不良的因素。我们旨在研究BMI对各种表型的急性心力衰竭(AHF)患者死亡风险的临床影响。
我们回顾性确定了4146例有AHF和BMI数据的登记患者。研究人群根据世界卫生组织亚太地区BMI分类进行分组:BMI<18.5kg/m²(体重过轻;n = 418),BMI 18.5 - 23kg/m²(理想体重;n = 1620),BMI 23 - 25kg/m²(超重;n = 828),BMI 25 - 30kg/m²(肥胖I;n = 1047),BMI≥30kg/m²(肥胖II;n = 233)。比较这5组患者的全因死亡风险。
在中位随访32个月期间,1732例患者(41.8%)死亡。与肥胖II患者相比,超重、理想BMI或体重过轻状态的患者死亡风险更高(超重:风险比[HR],1.606;95%置信区间[CI],1.016 - 2.539;p = 0.042)(理想BMI:HR,1.744;95% CI,1.112 - 2.734;p = 0.015)(体重过轻:HR,2.729;95% CI,1.686 - 4.417;p<0.001)。无论年龄、性别、高血压、糖尿病、缺血性心脏病、心房颤动和HF表型如何,BMI较低的患者死亡风险更高。此外,在579例患者的亚组中,使用血清胱抑素C数据计算的低肌肉指数(总肌肉质量/身高)与更高的死亡风险相关。
较低的BMI与AHF患者较高的死亡风险相关。在AHF中观察到这种肥胖悖论,无论合并症和HF表型如何。